Journal of Pediatric Medicine and Child Health
ISSN:
3108-2076 (Online)
DOI Prefix (Crossref): 10.67238
ABSTRACT
Background
Retinopathy of prematurity (ROP) is a leading cause of preventable childhood blindness, particularly in low- and middle-income countries. Omega-3 long-chain polyunsaturated fatty acids (LCPUFAs) play a critical role in retinal vascular and neuronal development and may influence the severity of ROP.
Objective
To evaluate the effect of enteral omega-3 LCPUFA supplementation on the incidence and severity of ROP in preterm low-birth-weight infants.
Methods
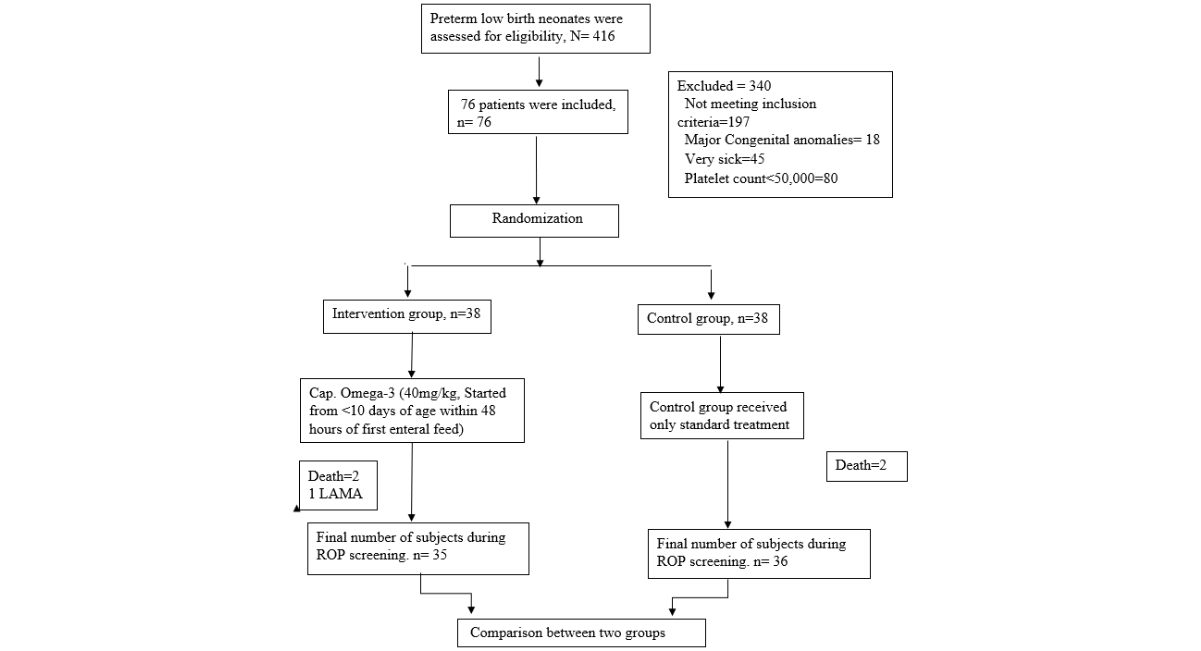
This randomized controlled trial was conducted at a tertiary care neonatal unit in Bangladesh between June to November 2023. Preterm neonates with gestational age >28 to <34 weeks and birth weight <1800 g were randomized to receive either enteral omega-3 supplementation (40 mg/kg/day of DHA) initiated within 48 hours of starting enteral feeds and continued for four weeks, or standard care without supplementation. ROP screening was performed according to national guidelines. Outcomes included overall ROP incidence, progression to severe or treatment-requiring ROP, and spontaneous regression.
Statistical analysis
Data were analyzed by Statistical Package for Social Science (SPSS 27.0 IBM Corporation, New York, USA).
Result
Among 76 enrolled infants, 71 completed follow-up (35 in the omega-3 group and 36 controls). Baseline neonatal and maternal characteristics were comparable between groups. The overall incidence of ROP did not differ significantly between the omega-3 and control groups (37.1% vs 41.7%, p=0.69). However, among infants who developed ROP, progression to severe ROP was significantly lower in the omega-3 group compared with controls (23.1% vs 60.0%, p=0.049), while spontaneous regression was significantly higher (76.9% vs 40.0%, p=0.049).
Conclusion
Enteral omega-3 supplementation does not reduce the overall incidence of ROP but significantly lowers the risk of severe, treatment-requiring disease and promotes spontaneous regression. Omega-3 LCPUFAs may serve as a supportive nutritional strategy to modulate ROP severity in preterm infants. Further multicenter studies are needed to determine optimal dosing and long-term outcomes.
Keywords: Retinopathy of Prematurity; Omega-3 Fatty Acids; Preterm Infants; Neonatal Nutrition
INTRODUCTION
Visual development during early life is a critical determinant of cognitive function, educational achievement, and overall quality of life. Disorders that disrupt vision at infancy therefore have consequences that extend far beyond childhood, often resulting in lifelong disability and social dependence [1]. Among preventable causes of childhood visual impairment, neonatal-onset conditions occupy a critical position, with Retinopathy of Prematurity (ROP)-a vasoproliferative disorder of the immature retina-remaining a leading cause of avoidable blindness among preterm infants [2]. The World Health Organization’s Vision 2020 program identified ROP as a leading cause of childhood blindness, particularly in low- and middle-income countries.
Retinopathy of Prematurity (ROP) emerges as a consequence of vascular and neural developmental interruption of retina in premature infants. Rather than a single disease entity, ROP reflects a spectrum of abnormal retinal vascular responses to extrauterine life. Its clinical manifestation ranges from spontaneous regression to rapidly progressive disease with permanent retinal damage and blindness. Importantly, the severity of ROP-not merely its presence-largely determines visual prognosis and the need for invasive treatment during infancy [3]. The prevalence of ROP ranges from 7-37% in different countries depending on the degree of prematurity and birth weight [4]. The rate of ROP has increased as the survival rate among preterm newborns has increased due to continuous improvement in neonatal care. Every year around 32,300 infants worldwide are diagnosed with irreversible vision impairment caused by ROP. Two sperate studies done in Banglaesh revealed the incidence of ROP was 19.5% and 31.9% [5-7].
The pathogenesis of ROP involves disruption of normal retinal vasculogenesis following premature birth. Exposure to an extrauterine environment alters oxygen regulation and angiogenic signaling, leading to delayed physiological vascular growth and, in some infants, subsequent pathological neovascularization [8]. The severity of ROP is therefore not determined by a single factor, but by complex interactions between gestational immaturity, postnatal exposures, and nutritional status [3].
Nutrition, particularly lipid nutrition, has emerged as a critical modifiable factor in early retinal development. Omega-3 Long-Chain Polyunsaturated Fatty Acids (LCPUFAs), notably Docosahexaenoic Acid (DHA) and Eicosapentaenoic Acid (EPA), are essential components of neuronal and retinal cell membranes [9]. During normal fetal development, the majority of DHA accretion occurs in the final trimester of pregnancy, a period that preterm infants do not complete. They also are born with low stores, and rely on dietary intake postnatally [10]. Breast milk DHA is often insufficient and variable, and in Bangladesh, low maternal omega-3 intake further increases the risk of deficiency in preterm neonates [11].
Experimental and clinical studies suggest that omega-3 LCPUFAs may attenuate several key mechanisms involved in ROP pathogenesis. Beyond their structural role, omega-3 fatty acids have been shown to influence biological pathways that are relevant to neonatal vascular disorders. Their anti-inflammatory and endothelial-stabilizing effects suggest a potential role in moderating aberrant vascular responses during retinal development [12]. Unlike pharmacological interventions, nutritional supplementation offers the advantage of early initiation, physiological integration, and feasibility within routine neonatal care [13].
Several experimental and clinical studies have indicated a potential protective role of omega-3 fatty acids in retinal vascular disorders, including ROP [13-15]. However, findings across studies have been heterogeneous, and data from resource-limited settings remain scarce. Moreover, many prior investigations have focused on parenteral lipid emulsions, which are not routinely available in all neonatal units, limiting their generalizability to everyday clinical practice in settings such as Bangladesh [15].
In Bangladesh, where prematurity and low birth weight is common, strategies aimed at reducing the severity of ROP are particularly relevant [16]. Enteral omega-3 supplementation represents a feasible and low-cost intervention that can be incorporated into standard feeding protocols [17]. However, evidence regarding its effectiveness in modifying ROP outcomes in this population is limited. The present randomized controlled trial therefore aimed to evaluate the effect of enteral omega-3 long-chain polyunsaturated fatty acid supplementation on the occurrence and severity of retinopathy of prematurity among preterm low-birth-weight infants admitted to a tertiary care neonatal unit in Bangladesh.
MATERIALS AND METHODS
This randomized controlled trial was conducted among preterm low-birth infants admitted to the Department of Neonatology, Bangladesh Shishu Hospital & Institute, Dhaka. Data collection was done from 1 st June, 2023 to 30 th November, 2023.
Preterm neonates of 0-8days with gestational age >28weeks to <34 weeks, having birth weight <1800 gram, and in whom enteral feeding has been started were included in the study. Infants with major congenital anomalies, presence of other eye conditions like cataracts or corneal opacity, any severe bleeding manifestations ie. interventricular hemorrhage, gastrointestinal bleeding, infants with platelet count <50,000 cmm, infants in mechanical ventilator, history of taking omega 3 supplementation in mother were excluded from the study.
STUDY PROCEDURE
Preterm neonates with gestational age >28 to <34 weeks were enrolled using simple random sampling. Block randomization (1:1) was performed using a lottery method with sealed envelopes.
Gestational age was assessed using the modified New Ballard Score and maternal last menstrual period; in case of discrepancy, the New Ballard Score was used. Baseline demographic and clinical data were collected using a structured questionnaire. Both groups received enteral nutrition with maternal or donor breast milk, with similar feed advancement protocols.
Neonates in the intervention group received enteral omega-3 supplementation at a dose of 40 mg/kg/day DHA, initiated within 48 hours of the first enteral feed and continued for 4 weeks. Omega-3 was administered orally or via nasogastric tube along with breast milk. The control group received standard neonatal care without supplementation.
All enrolled neonates underwent Retinopathy of Prematurity (ROP) screening at the National Institute of Ophthalmology, Agargaon, following national guidelines. The first screening was performed at 20 days of life for neonates ≤30 weeks’ gestation and at 30 days for those >30 weeks. Screening was conducted by an ophthalmologist using binocular indirect ophthalmoscopy after pharmacologic pupillary dilation and topical anesthesia.
ROP was classified by stage, zone, and presence of plus disease. Follow-up examinations were scheduled according to disease severity. Treatment (laser photocoagulation and/or intravitreal bevacizumab) was provided within 48 hours for treatment-requiring ROP. Screening continued until complete retinal vascularization or full regression of ROP.
Study Flow Chart
Statistical analysis
All the data were processed and analyzed by SPSS 27.0. Data were expressed as numbers and percentages for categorical variables or as means and ranges for quantitative variables. All data was presented in a suitable table or graph. Categorical data were analyzed by the Chi-square (χ2) test and Fisher’s exact test. Student t-test was used for continuous data. For all statistical tests p-value of less than 0.05 was considered statistically significant
Ethical Consideration
Before the commencement of the study, the research protocol was approved by the Ethical Review Committee (ERC) of Bangladesh Shishu Hospital & Institute, Dhaka. Informed and written consent was obtained from the legal guardians of each child. It was assured that all information and records would be kept confidential. They were at liberty to withdraw from the study at any time if they desired, it did not affect the management of the patients.
RESULTS
Initially, a total of 76 patients were included in the study. The Omega-3 and control groups each included 38 participants. Gender distribution was in the Omega-3 group versus control group, with no significant difference. Birth weights and gestational age, whether analyzed categorically or as means, were also comparable between groups (birth weight p = 0.354 and 0.472; gestational age p = 0.123). The mean duration of oxygen therapy was 12.47 ± 2.21 days in the Omega-3 group and 12 ± 2.46 days in the control group, with no significant difference between groups (p = 0.38). Additionally, maternal and delivery-related variables-including parity, gestational diabetes, antenatal corticosteroids, prolonged rupture of membranes, maternal diabetes or hypertension, antepartum hemorrhage, place and mode of delivery, and multiple births-showed no significant differences (Table I).
|
Variables |
Omega-3 Group (n=38) |
Control Group (n=38) |
p-value |
|
Frequency (%) |
Frequency (%) |
||
|
Gender |
|||
|
Male |
21 (55.3) |
26 (68.4) |
c0.238 ns |
|
Female |
17 (44.7) |
12 (31.6) |
|
|
Birth weight (gm) |
|||
|
<1000 |
4 (10.5) |
7 (18.4) |
f0.354 ns |
|
1000-1499 |
26 (68.4) |
20 (52.6) |
|
|
1500-1799 |
8 (21.1) |
11 (28.9) |
|
|
Mean±SD |
1332.47±185.05 |
1288.68±242.58 |
t0.472 ns |
|
Gestational age (weeks) |
|||
|
>28-<30 weeks |
5 (13.2) |
8 (21.1) |
c0.658 ns |
|
30-<32 |
10 (26.3) |
9 (23.7) |
|
|
32-<34 |
23 (60.5) |
21 (55.3) |
|
|
Mean±SD |
31.60±1.38 |
31.10±1.41 |
t0.123 ns |
|
Total oxygenation therapy (mean days) |
12.47±2.21 |
12±2.46 |
t0.381 ns |
Table I: Baseline characteristics of the infants and their mothers enrolled in the study (N=76)
p-value reached through cchi-square test for categorical variables and ffisher exact test where the expected value was <5 in ≥20% cells. p-value reached through tunpaired t-test for continuous variables.
ns = non-significant; s = significant
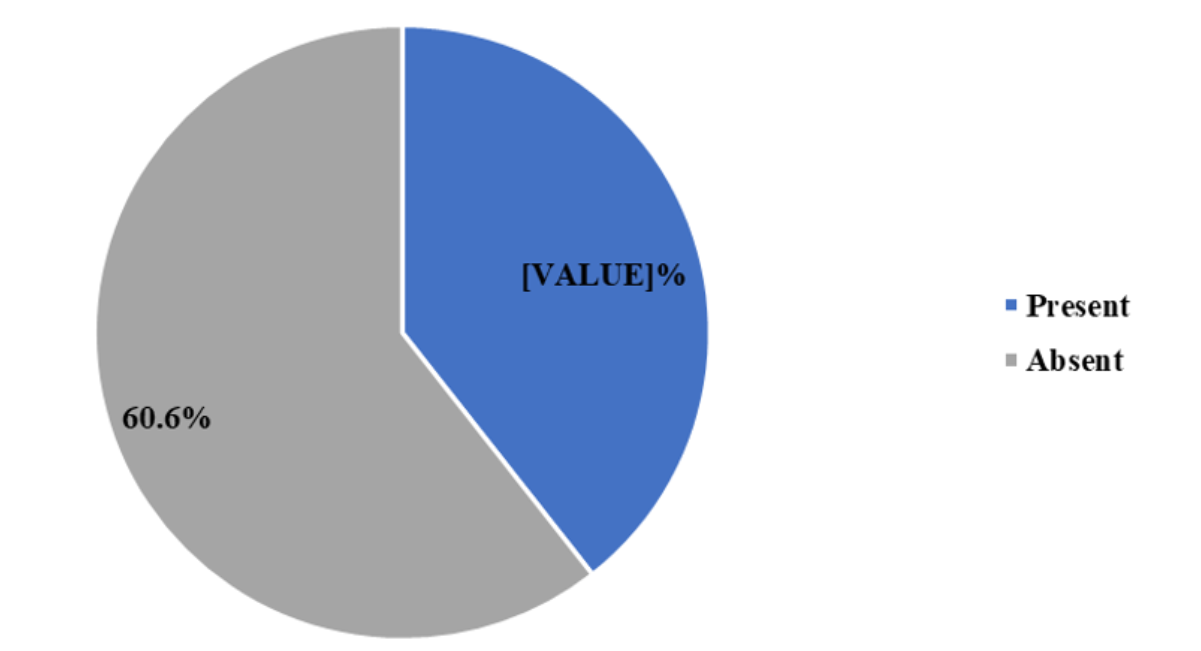
Figure 1: Overall incidence of ROP among all the study participants (N=71)
Among 76 participants who were initially enrolled only 71 who attened the final ROP screening. Among them, 39.4% developed ROP, while 60.6% showed no signs of the condition. (Fig-1)
In the Omega-3 group, 3 of 35 participants (8.5%) developed severe ROP, compared to 9 of 36 (25%) in the control group. Spontaneous regression occurred in 10 participants (28.6%) in the Omega-3 group versus 6 (16.7%) in the control group, while 22 (65.9%) and 21 (58.3%) participants in the intervention and control groups, respectively, did not develop ROP. None of these differences were statistically significant (severe ROP p = 0.059; spontaneous regression p = 0.064; no ROP p = 0.646) (Table 2).
|
ROP |
Omega-3 Group (n=35) |
Control Group (n=36) |
p-value |
|
Severe ROP |
3 (8.5) |
9 (25) |
c0.059ns |
|
Spontaneous Regression of ROP |
10 (28.6) |
6 (16.7) |
c0.064ns |
|
No ROP |
22 (62.9) |
21 (58.3) |
c0.646ns |
Table 2: Comparison of the development of ROP between two groups (N=71)
p-value reached through cchi-square test for categorical variables
ns = non-significant; s = significant
Among participants who developed ROP, 3 of 13 cases (23.1%) in the intervention group progressed to severe ROP, compared to 9 of 15 cases (60%) in the control group (p = 0.049). Spontaneous regression occurred in 10 participants (76.9%) in the intervention group versus 6 (40%) in the control group, also showing a significant difference (p = 0.049) (Table III).
|
ROP |
Omega-3 Group (n=13) |
Control Group (n=15) |
p-value |
|
Severe ROP |
3 (23.1) |
9 (60) |
c0.049s |
|
Spontaneous Regression |
10 (76.9) |
6 (40) |
c0.049s |
Table 3: Comparison of type of ROP among ROP patients of two groups (N=28)
p-value reached through cchi-square test for categorical variables
ns = non-significant; s = significant
The distribution of cases across various stages, presenting frequencies and percentages for each stage. Stage 1 comprises the highest number of cases, with 13 instances, constituting 46.4% of the total. Following this, APROP exhibits 7 cases, representing 25% of the total, while Stage 3 and stage 2 occurrences were 14.2% and 10.7% respectively and 1 case in Stage 5 ROP (3.6%) (Table 4)
There was no statistically significant difference in ROP frequency between the omega-3 and control groups across any gestational age category (all p > 0.05). Although ROP tended to be more frequent at lower gestational ages-particularly in the control group—these differences were not significant, likely due to small subgroup sample sizes. Thus, omega-3 supplementation did not show a gestational age–specific effect on ROP in this study (Table 4 ).
|
Gestational age (weeks) |
ROP |
p-value |
|
|
Omega-3 Group (n=13) |
Control Group (n=15) |
||
|
Frequency (%) |
Frequency (%) |
||
|
>28-<30 |
4 (11.4) |
7 (19.4) |
c0.351ns |
|
30-<32 |
6 (17.1) |
7 (19.4) |
c0.802ns |
|
32-<34 |
3 (8.6) |
1 (2.8) |
f0.296ns |
Table 4: Comparison of ROP incidence according to gestational age (N=28)
p-value reached through cchi-square test for categorical variables and ffisher exact test where expected value was <5 in ≥20% cells. ns = non-significant; s = significant
DISCUSSION
This study provides insight into the potential role of Omega-3 supplementation in modulating the course of ROP in preterm infants. Baseline characteristics-including sex distribution, gestational age, birth weight, and maternal factors-were similar between the Omega-3 supplemented and control groups, reducing the likelihood of confounding effects on study outcomes. Comparable baseline profiles are crucial for ensuring that any observed differences in ROP incidence or severity can be attributed to the intervention rather than underlying demographic or clinical disparities. Similar observations have been reported in three other randomized controlled trials evaluating Omega-3 supplementation in preterm infants, which also found no significant differences in baseline characteristics between study groups [15,17,18]. This consistency across studies strengthens the validity of the current findings and supports the conclusion that differences in ROP outcomes are likely related to Omega-3 supplementation rather than variations in neonatal or maternal factors. This homogeneity ensures that any differences observed in outcomes are likely attributable to the intervention rather than underlying demographic or clinical disparities.
The overall incidence of ROP in the study population was 39.4%, which is slightly higher than figures reported in larger cohort studies [6,19]. This difference may be explained by this may reflect the smaller sample size and the high-risk nature of the study population. When comparing groups, the Omega-3 supplemented group showed a modest reduction in total ROP cases compared to controls; however, this difference was not statistically significant. This indicates that while enteral or dietary Omega-3 may contribute to retinal development, it may be insufficient on its own to prevent the onset of ROP [17,20,21]. These results are consistent with prior studies examining oral or enteral Omega-3 supplementation, which similarly reported minimal impact on overall ROP incidence. In contrast, trials utilizing parenteral administration of Omega-3 have demonstrated significant reductions in ROP, emphasizing that higher bioavailable doses may be necessary to achieve a protective effect [13,15].
Importantly, Omega-3 supplementation appears to have a meaningful impact on the progression and resolution of ROP, even if it does not significantly reduce the overall incidence of the disease. In the current study, infants in the intervention group who developed ROP were less likely to progress to severe or treatment-requiring stages compared to controls. Moreover, spontaneous regression occurred more frequently in the Omega-3 group than in the control group, a difference that was statistically significant. These findings suggest that Omega-3 fatty acids may support retinal development by enhancing vascular stability and reducing oxidative stress, creating conditions favorable for natural disease resolution, even if initial disease onset is not prevented [15,17,20]. All previous studies using parenteral Omega-3 supplementation have reported reductions in ROP severity and enhanced spontaneous regression [17,21]. However, findings regarding enteral Omega-3 supplementation are inconsistent; some trials have demonstrated significant reductions in severe ROP, while others found no significant effect [13,14,21]. Overall, these findings indicate that Omega-3 may not prevent the onset of ROP but can positively modulate its clinical course, promoting spontaneous regression and potentially reducing the need for therapeutic interventions.
These results have practical implications. While Omega-3 supplementation may not serve as a primary preventive strategy against ROP, it could reduce the need for invasive treatments and associated complications by promoting regression and limiting progression [8,14,15,20,21]. This highlights the potential value of nutritional interventions as an adjunct to standard neonatal care. Future studies should explore optimized dosing strategies, the comparative effectiveness of enteral versus parenteral administration, and the long-term visual outcomes associated with early Omega-3 supplementation.
CONCLUSION
This study concluded that Omega-3 supplementation does not reduce the overall incidence of ROP; however, it significantly lowers the risk of severe, treatment-requiring ROP and promotes spontaneous regression. These findings suggest a supportive role for Omega-3 in retinal vascular development, potentially reducing the need for interventions. Further research with optimized dosing and administration routes is warranted to confirm its clinical benefits.
LIMITATIONS
It is important to note that this study has some limitations that need to be considered. Firstly, the research was carried out at only one institute, so the findings may not be generalized. We could not do DHA and EPA levels of breast milk and blood before the supplementation. However, future trials with a larger number of patients as well as longer duration are needed to validate the findings of this study.
RECOMMENDATIONS
From this study, we can recommend that supplementation of omega-3 LCPUFA may prevent the occurrence of severe ROP. However, future trials with a larger number of patients as well as longer duration are needed to validate the findings of this study.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the contribution of Dr. Nasima Jahan, (Junior Consultant, National Institute of Ophthalmology), Prof. Monir Hossain (Professor, Bangladesh Shishu Hospital & Institute), Prof. Mahfuza Shirin (Professor, Bangladesh shishu Hospital & Institute), Dr. Akhand Tanzih Sultana, (Associate Professor, Bangladesh Shishu Hospital and Institute) and Dr. Nishat Sharmin, MD, (Dept of Neonatology, Bangladesh Shishu Hospital & Institute) for their contribution in data analysis and logistic support for this study.
DECLARATION OF CONFLICTING INTERESTS
There is no conflict of interest.
FUNDING AGENCY
This work has been funded by Bangladesh Neonatal Forum (BNF), Dhaka, Bangladesh.
CONTRIBUTION OF AUTHORS
Dr. Salma Afroz performed the implementation of the project, data collection, interpretation of data and writing this article. Prof. Md. Mahbubul Hoque, contributed in conception, supervision and drafting the article. Assoc. Prof Liton Chandra Saha revised it critically and helped in data interpretation and analysis.
REFERENCES
- Chorna O, Corsi G, Del Secco S, Bancale A, Guzzetta A. Correlation between early visual functions and cognitive outcome in infants at risk for cerebral palsy or other neurodevelopmental disorders: a systematic review. Children. 2024;11(6):747. [Crossref] [Google Scholar] [PubMed]
- Shrestha JB, Gautam Adhikari P, Shrestha GS. Causes of blindness and visual impairment among children studying in schools for the blind in central development region of Nepal. Nepal. Med. J. 2021;5(1):542-545. [Crossref] [Google Scholar]
- Huang D, Liu Z, Deng Y. Retinopathy of Prematurity (ROP): An Overview of Biomarkers in Various Samples for Prediction, Diagnosis, and Prognosis. Clinical Ophthalmology. 2025:1515-1530. [Crossref] [Google Scholar] [PubMed]
- Fares A, Abdelmonaim S, Sayed D, Sadek S, Abdulrazek A, Helmy Y, et al. Validation of WINROP algorithm as screening tool of retinopathy of prematurity among Egyptian preterm neonates. Eye. 2024;38(8):1562-156. [Crossref] [Google Scholar] [PubMed]
- Hariharan L, Gilbert CE, Quinn GE, Barg FK, Lomuto C, Quiroga A, et al. Reducing blindness from retinopathy of prematurity (ROP) in Argentina through collaboration, advocacy and policy implementation. Health Policy Plan. 2018;33(5):654–665. [Crossref] [Google Scholar] [PubMed]
- Mannan MA. Frequency and risk factors of retinopathy of prematurity among preterm neonates in a tertiary care hospital of Bangladesh. J. Clin. Pediatr. Neonatol. 2023;3(1):11-17. [Crossref] [Google Scholar]
- Rahman M, Saha L, Hoque M, Hossain M, Yasmeen BH. Retinopathy of prematurity: Bangladesh perspective. North. Int. Med. Coll. J. 2021;11:447–452. [Crossref] [Google Scholar]
- Cavallaro G, Filippi L, Bagnoli P, La Marca G, Cristofori G, Raffaeli G, et al. The pathophysiology of retinopathy of prematurity: an update of previous and recent knowledge. Acta ophthalmologica. 2014;92(1):2-10. [Crossref] [Google Scholar] [PubMed]
- Malamas A, Chranioti A, Tsakalidis C, Dimitrakos SA, Mataftsi A. The omega-3 and retinopathy of prematurity relationship. Int. J. Ophthalmol. 2017;10(2):300. [Crossref] [Google Scholar] [PubMed]
- Smith SL, Rouse CA. Docosahexaenoic acid and the preterm infant. Matern. Health Neonatol. Perinatol. 2017;3:22. [Crossref] [Google Scholar] [PubMed]
- Kim H, Kang S, Jung BM, Yi H, Jung JA, Chang N. Breast milk fatty acid composition and fatty acid intake of lactating mothers in South Korea. Br. J. Nutr. 2017;117(4):556–561. [Crossref] [Google Scholar] [PubMed]
- Shen S, Yan G, Cao Y, Zeng Q, Zhao J, Wang X, et al. Dietary supplementation of n-3 PUFAs ameliorates LL37-induced rosacea-like skin inflammation via inhibition of TLR2/MyD88/NF-κB pathway. Biomed. Pharmacother. 2023;157:11409. [Crossref] [Google Scholar] [PubMed]
- Beken S, Dilli D, Fettah ND, Kabataş EU, Zenciroğlu A, Okumuş N. The influence of fish-oil lipid emulsions on retinopathy of prematurity in very low birth weight infants: A randomized controlled trial. Early Hum. Dev. 2014;90(1):27-31. [Crossref] [Google Scholar] [PubMed]
- Hellström A, Nilsson AK, Wackernagel D, Pivodic A, Vanpee M, Sjöbom U, et al. Effect of enteral lipid supplement on severe retinopathy of prematurity: a randomized clinical trial. JAMA pediatrics. 2021;175(4):359-367. [Crossref] [Google Scholar] [PubMed]
- Tu CF, Lee CH, Chen HN, Tsao LY, Chen JY, et al. Effects of fish oil-containing lipid emulsions on retinopathy of prematurity in very low birth weight infants. Pediatr. Neonatol. 2020;61(2):224–230. [Crossref] [Google Scholar] [PubMed]
- Hussain AHME, Islam K, Kabir ANME. National Guidelines for Screening and Management of Retinopathy Of Prematurity. 2022.
- Yang R, Ding H, Shan J, Li X, Zhang J, Liu G, et al. Association of fish oil containing lipid emulsions with retinopathy of prematurity: a retrospective observational study. BMC pediatrics. 2022 Mar 2;22(1):113. [Crossref] [Google Scholar] [PubMed]
- Khalesi N, Bordbar A, Khosravi N, Kabirian M, Karimi A. The efficacy of Omega-3 supplement on prevention of retinopathy of prematurity in premature infants: A randomized double-blinded controlled trial. Curr. Pharm. Des. 2018;24(17):1845–1848. [Crossref] [Google Scholar] [PubMed]
- Akther M, Tabrez MS, Choudhury N, Moni SC, Dey SK, Jahan I, et al. Postnatal weight gain as a predictor of retinopathy of prematurity in preterm babies. J. Clin. Neonatol.. 2022;11(2):102-106. [Crossref] [Google Scholar]
- Pawlik D, Lauterbach R, Walczak M, Hurkała J, Sherman MP. Fish‐oil fat emulsion supplementation reduces the risk of retinopathy in very low birth weight infants: a prospective, randomized study. J. Parenter. Enteral Nutr. 2014;38(6):711-716. [Crossref] [Google Scholar] [PubMed]
- Bernabe‐García M, Villegas‐Silva R, Villavicencio‐Torres A, Calder PC, Rodríguez‐Cruz M, Maldonado‐Hernández J, et al. Enteral docosahexaenoic acid and retinopathy of prematurity: a randomized clinical trial. J. Parenter. Enteral Nutr. 2019;43(7):874-882. [Crossref] [Google Scholar] [PubMed]
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 25-35 Days |
Peer Review Feedback |
| 45-60 Days | Total article processing time |
Journal Flyer