Journal of Pediatric Medicine and Child Health
ISSN:
3108-2076 (Online)
DOI Prefix (Crossref): 10.67238
ABSTRACT
Background
Pediatric cancer is increasingly recognized as a significant public health concern in Africa. Despite advances in childhood cancer diagnosis and treatment globally, African countries continue to experience poor survival outcomes due to delayed diagnosis, inadequate oncology infrastructure, limited surveillance systems, and restricted access to essential cancer care services. However, evidence on the epidemiology and emerging trends of pediatric cancers across Africa remains fragmented.
Objective
This scoping review aimed to map and synthesize the available evidence on the epidemiology, incidence trends, geographic distribution, risk factors, surveillance gaps, and priorities for the prevention and control of pediatric cancers in Africa.
Methods
A scoping review methodology guided by the Arksey and O’Malley framework, Joanna Briggs Institute guidance, and PRISMA-ScR recommendations was employed. Literature searches were conducted across PubMed/MEDLINE, Scopus, Web of Science, Google Scholar, African Journals Online, and institutional sources including WHO and IARC. Eligible studies focused on pediatric cancers among individuals aged 0–19 years in African settings and addressed epidemiological patterns, surveillance systems, treatment challenges, or prevention strategies.
Results
Sixty-two evidence sources were included in the review. Leukemias, lymphomas, Burkitt lymphoma, Wilms tumor, retinoblastoma, and Kaposi sarcoma were the most frequently reported pediatric malignancies across Africa. Infectious diseases, including HIV, Epstein–Barr virus, malaria, and Kaposi sarcoma-associated herpesvirus, were strongly associated with several childhood cancers. Major barriers to effective pediatric cancer control included weak cancer registries, limited diagnostic infrastructure, workforce shortages, treatment abandonment, and socioeconomic inequalities. Nevertheless, growing regional collaborations and WHO-led initiatives indicate increasing momentum toward strengthening pediatric oncology systems across the continent.
Conclusion
Pediatric cancer represents an emerging and underrecognized health burden in Africa. Strengthening cancer surveillance, early detection systems, diagnostic capacity, oncology workforce development, and equitable access to treatment is essential for improving childhood cancer outcomes and supporting evidence-based pediatric cancer control strategies across African settings.
Keywords: Pediatric Cancer, Childhood Malignancies, Africa, Cancer Epidemiology, Cancer Surveillance, Burkitt Lymphoma, Pediatric Oncology
INTRODUCTION
Childhood cancer is increasingly recognized as a major global public health concern, contributing substantially to the morbidity and mortality of children and adolescents worldwide. According to the World Health Organization (WHO, 2025), approximately 400,000 children and adolescents aged 0–19 years develop cancer annually, with leukemia, brain tumors, lymphomas, and solid tumors being the most common malignancies. Although survival outcomes for pediatric cancers now exceed 80% in many high-income countries owing to advances in early diagnosis, multimodal treatment, supportive care, and strengthened oncology systems, substantial disparities persist across Low- And Middle-Income Countries (LMICs), particularly in Africa [1,2].
In many African settings, survival rates for childhood cancers remain below 30%, largely due to delayed diagnosis, inadequate treatment infrastructure, treatment abandonment, shortages of specialized personnel, weak referral systems, and limited access to essential cancer medicines [3,4]. These inequities have intensified international concerns regarding the emerging burden of pediatric cancers in resource-constrained settings and the urgent need for context-specific prevention and control strategies across the continent.
Recent international registry-based analyses have reported increasing or increasingly recognized incidence patterns of childhood cancers across several regions globally [5,9]. The International Incidence of Childhood Cancer project, coordinated by the International Agency for Research on Cancer (IARC), demonstrated substantial geographic variation in pediatric cancer incidence and highlighted major limitations in cancer surveillance capacity across many LMICs, including African countries [5]. Similarly, simulation-based global estimates suggested that a considerable proportion of childhood cancer cases in sub-Saharan Africa may remain undiagnosed or unrecorded because of inadequate registry systems, limited diagnostic infrastructure, and restricted access to pediatric oncology services [1]. Population-based registry studies from Zimbabwe, Uganda, Malawi, and Ghana have further reported changing incidence patterns and increasing recognition of pediatric malignancies over time [6,7,8,10].
The epidemiology of pediatric cancers in Africa is influenced by the complex interaction of demographic, infectious, environmental, socioeconomic, and health system factors. Leukemias, lymphomas, Wilms tumors, retinoblastoma, Kaposi sarcoma, and Burkitt lymphoma are among the most frequently reported pediatric malignancies across the continent [11,12]. Infectious diseases play a particularly important role in shaping the patterns of pediatric cancers in Africa. Human immunodeficiency virus (HIV), Epstein-Barr virus (EBV), malaria, and Kaposi Sarcoma-associated Herpes virus (KSHV) have all been associated with an increased risk of specific childhood malignancies, particularly Burkitt lymphoma and Kaposi sarcoma [13,14,15]. Emerging evidence has highlighted important associations between malaria endemicity and endemic Burkitt lymphoma in several African regions [16,17,18].
In addition to biological and infectious determinants, structural and socioeconomic barriers significantly influence pediatric cancer outcomes across Africa. Low public awareness, delayed care-seeking behavior, weak referral systems, inadequate pathology services, shortages of pediatric oncology specialists, and financial hardship continue to contribute to delayed diagnosis, advanced-stage presentation, treatment interruption, and treatment abandonment [18,19,20]. Socioeconomic inequalities and limited caregiver health literacy further complicate access to timely and effective cancer care in many African settings [22,23]. In addition, major disparities in cancer registration capacity, pathology infrastructure, staging systems, and reporting quality continue to obscure the true burden of pediatric cancers and limit reliable regional comparisons across the continent [24,25]
Recognizing these challenges, the WHO launched the Global Initiative for Childhood Cancer to improve survival and quality of care for children with cancer through strengthened health systems, expanded access to essential medicines, enhanced early detection, improved cancer registration systems, and implementation of context-specific pediatric oncology strategies [26,27]. Increasing regional efforts aimed at strengthening pediatric oncology networks, improving diagnostic capacity, and expanding cancer surveillance systems across Africa further reflect the growing recognition of childhood cancer as an emerging continental health priority [28,29].
Despite these advances, the available evidence on pediatric cancers in Africa remains fragmented across countries, cancer types, and isolated registry-based studies. The existing literature has largely focused on single-country experiences or specific malignancies, with limited continent-wide synthesis of epidemiological trends, geographic distribution, infectious and socioeconomic risk factors, surveillance limitations, and prevention and control priorities. Although international cancer surveillance reports and global reviews have contributed important insights into childhood cancer epidemiology, African pediatric oncology data remain underrepresented, heterogeneous, and incompletely integrated within the broader literature. This fragmented evidence base poses important challenges for policy development, resource allocation, early detection planning, cancer control programming, and pediatric oncology system strengthening across African settings.
Given the evolving landscape of pediatric cancer recognition and control efforts in Africa, there is a need to comprehensively map the breadth and distribution of the existing evidence while identifying major epidemiological, surveillance, and health system gaps. Therefore, this scoping review aimed to map and synthesize the literature on the emerging burden of pediatric cancers in Africa, with particular emphasis on epidemiological trends, incidence patterns, geographic distribution, risk factors, surveillance gaps, and prevention and control priorities. This review further sought to identify key evidence deficiencies and highlight the implications for pediatric cancer prevention, early detection strategies, research prioritization, and health system strengthening across African settings.
METHODS
Study Design
We conducted a scoping review to map and synthesize the available evidence on the emerging burden of pediatric cancers in Africa, with emphasis on epidemiological trends, incidence patterns, geographic distribution, risk factors, surveillance gaps, and priorities for prevention and control. A scoping review approach was considered appropriate because the existing literature on pediatric cancers in Africa is heterogeneous, fragmented across countries and cancer types, and characterized by variations in study design, registry quality, and reporting systems. The review methodology was guided by the methodological framework for scoping reviews proposed by Arksey and O’Malley (2005) and further refined by Levac et al. (2010) and the Joanna Briggs Institute (JBI) guidance for scoping reviews. The reporting of the review process was additionally informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist.
Search Strategy
A comprehensive literature search was conducted to identify studies reporting on pediatric cancer epidemiology, incidence trends, surveillance systems, risk factors, treatment challenges, and prevention and control strategies in African settings. Searches were performed across major electronic databases, including PubMed/MEDLINE, Scopus, Web of Science, Google Scholar, and African Journals Online. Additional records were identified through manual screening of reference lists of eligible articles and relevant institutional reports.
The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords related to childhood cancers and African settings. Core search terms included combinations of: pediatric cancer, childhood cancer, childhood malignancies, pediatric oncology, cancer incidence, epidemiology, cancer registry, Burkitt lymphoma, retinoblastoma, Wilms tumor, leukemia, Africa, sub-Saharan Africa, prevention, control, and surveillance. Boolean operators were used to refine searches and improve retrieval sensitivity. The search process was supplemented with reports and publications from the World Health Organization (WHO), International Agency for Research on Cancer (IARC), African Cancer Registry Network (AFCRN), and other relevant global cancer surveillance initiatives.
Eligibility Criteria
Studies were included if they met the following criteria:
- reported on pediatric or childhood cancers in individuals aged 0–19 years.
- focused on African countries or populations.
- addressed cancer incidence, epidemiological trends, geographic distribution, risk factors, cancer registration, survival, treatment barriers, surveillance systems, or prevention and control strategies.
- were observational studies, registry-based analyses, systematic reviews, scoping reviews, policy reports, or institutional surveillance publications; and
- were published in the English language.
Studies focusing exclusively on adult cancers, non-African populations, experimental laboratory studies without epidemiological relevance, conference abstracts lacking sufficient methodological detail, and articles with inaccessible full texts were excluded from the review. Where appropriate, landmark historical studies and major international cancer surveillance reports were retained because of their relevance to pediatric cancer epidemiology and registry development in Africa.
Study Selection
All retrieved records were screened in stages. After removing duplicates, titles and abstracts were reviewed for relevance to the objectives of the review. The full texts of potentially eligible articles were subsequently assessed against the inclusion criteria. We conducted the screening and selection process iteratively to ensure consistency with the review objectives and to capture studies addressing epidemiology, surveillance systems, infectious and socioeconomic determinants, treatment challenges, and pediatric oncology control efforts across African settings.
Data Extraction and Synthesis
Relevant data were extracted from the included studies using a structured data charting approach. The extracted information included author details, year of publication, country or region of study, study design, study population, cancer type, incidence patterns, epidemiological findings, identified risk factors, surveillance characteristics, treatment and health system challenges, and key prevention or control strategies.
The findings were synthesized descriptively and organized thematically according to major domains emerging from the literature. These domains included epidemiological trends and incidence patterns, geographic distribution of pediatric cancers, infectious and environmental risk factors, cancer registration and surveillance gaps, delayed diagnosis and treatment barriers, treatment abandonment, and priorities for pediatric cancer prevention and control across African settings. Given the heterogeneity of study designs, outcomes, and reporting approaches, a quantitative meta-analysis was not undertaken.
Quality Considerations
Consistent with the scoping review methodology, a formal risk-of-bias assessment was not performed. However, the methodological characteristics of the included studies, registry completeness, surveillance limitations, and reporting quality were considered during the interpretation and synthesis of the findings. Greater emphasis was placed on population-based registry studies, multicenter analyses, WHO and IARC reports, and studies with clearly described methodologies and surveillance frameworks.
RESULTS
Study Selection
A literature search across PubMed/MEDLINE, Scopus, Web of Science, Google Scholar, African Journals Online (AJOL), and institutional sources, including the World Health Organization (WHO), International Agency for Research on Cancer (IARC), and African Cancer Registry Network (AFCRN), identified 1,284 records. An additional 46 records were identified through manual searches of reference lists, institutional reports, and relevant gray literature sources, resulting in 1,330 total records.
After removing duplicates, 1,012 records remained for title and abstract screening. During this stage, 842 records were excluded because they focused exclusively on adult cancers, non-African populations, laboratory-based studies without epidemiological relevance, unrelated oncologic conditions, or lacked sufficient relevance to pediatric cancer epidemiology, surveillance, prevention, or control.
A total of 170 full-text articles were assessed for eligibility. Of these, 108 articles were excluded for reasons including insufficient pediatric-specific data, absence of African study populations, limited methodological detail, duplicate reporting of registry findings, or lack of relevance to the objectives of the review.
Ultimately, 62 sources of evidence were included in the final synthesis. These included population-based cancer registry studies, observational epidemiological studies, multicenter pediatric oncology investigations, systematic and scoping reviews, WHO and IARC surveillance reports, pediatric oncology system-strengthening studies, and selected landmark publications relevant to pediatric cancer epidemiology and control in Africa.
The included literature spanned multiple African regions and addressed a broad range of pediatric malignancies, including leukemia, lymphoma, Burkitt lymphoma, Kaposi sarcoma, Wilms tumor, retinoblastoma, and central nervous system tumors. The study selection process is summarized in the PRISMA flow diagram (Figure 1).
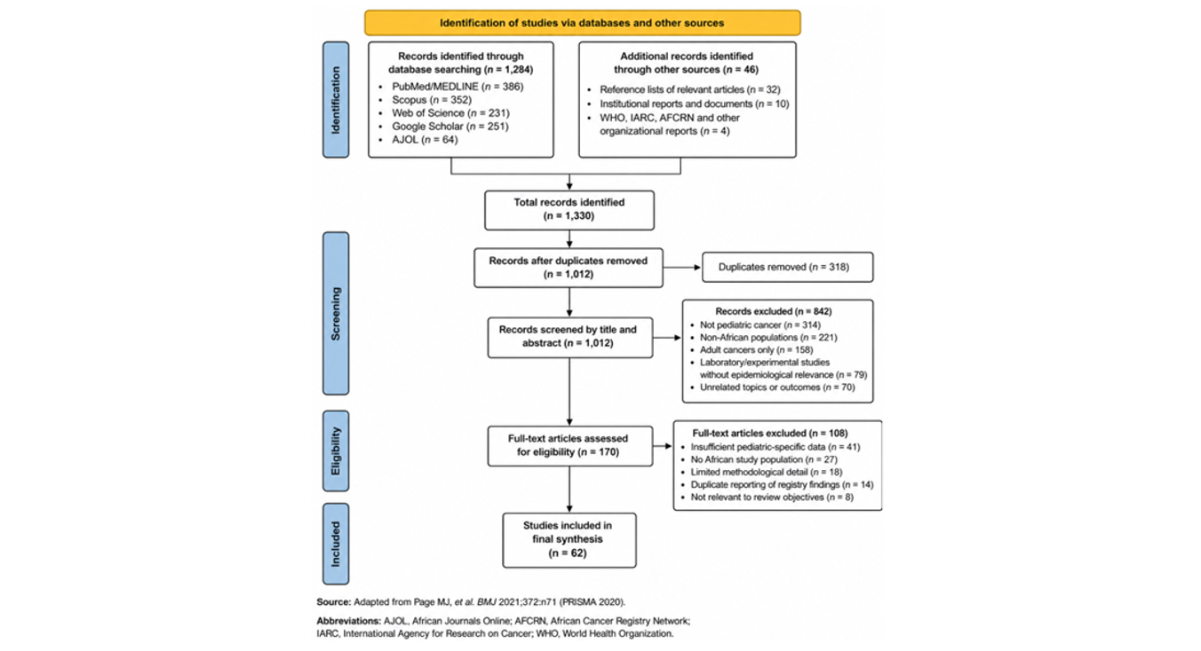
Figure 1: PRISMA 2020 flow diagram of study selection for the scoping review
Characteristics of Included Studies
A total of 62 evidence sources were included in this scoping review, comprising population-based cancer registry studies, retrospective hospital-based studies, observational epidemiological investigations, multicenter collaborative studies, systematic and scoping reviews, methodological reports, policy documents, and international surveillance publications. The representative characteristics of the selected studies are presented in Table 1, while the complete description of all included studies is provided in Supplementary Table 1.
The included literature covered multiple African regions, with studies originating predominantly from sub-Saharan Africa. Frequently represented countries included Uganda, Zimbabwe, Ghana, Kenya, South Africa, Nigeria, Zambia, Malawi, Senegal, Mali, and Ethiopia. Several multicountry investigations additionally incorporated data from regional and international pediatric oncology collaborations, such as the African Cancer Registry Network (AFCRN), the International Incidence of Childhood Cancer (IICC) project coordinated by the International Agency for Research on Cancer (IARC), and the Franco-African Pediatric Oncology Group (GFAOP).
Most studies have focused on pediatric cancer epidemiology, incidence trends, survival outcomes, cancer registration systems, infectious risk factors, treatment barriers, and health system limitations. Registry-based incidence analyses constituted a substantial proportion of the included evidence and provided important insights into temporal changes in childhood cancer patterns across African settings. Studies from Uganda and Zimbabwe reported increasing incidence trends over time, while simultaneously highlighting limitations in diagnostic infrastructure and surveillance systems [6,30,31].
Leukemias, lymphomas, Burkitt lymphoma, Wilms tumor, retinoblastoma, and Kaposi sarcoma emerged as the most frequently reported pediatric malignancies across the included studies. Several investigations emphasized the distinct epidemiological profile of pediatric cancers in Africa, particularly the influence of infectious diseases such as human immunodeficiency virus (HIV), Epstein–Barr Virus (EBV), malaria, and Kaposi Sarcoma-associated Herpesvirus (KSHV) on childhood cancer occurrence patterns. Multiple studies from Uganda, Malawi, Zambia, Ghana, and South Africa explored associations between infectious exposures and Burkitt lymphoma or Kaposi sarcoma, underscoring the importance of infection-related carcinogenesis within African pediatric oncology settings. Several included studies further examined the structural determinants influencing pediatric cancer outcomes across African health systems. Commonly reported challenges included delayed diagnosis, treatment abandonment, limited pathology infrastructure, shortages of pediatric oncology specialists, and restricted access to essential medicines, financial hardship, weak referral pathways, and caregiver-related socioeconomic burdens. Emerging literature has additionally highlighted efforts aimed at strengthening pediatric oncology systems through improved staging frameworks, regional collaborations, enhanced cancer registration systems, and implementation of the WHO Global Initiative for Childhood Cancer.
Methodological approaches varied considerably across the included literature. While some studies utilized population-based cancer registries and multicenter surveillance systems, others relied on single-center retrospective analyses or hospital-based datasets. Several authors have identified persistent concerns regarding incomplete cancer registration, underdiagnosis, inconsistent pathology classification, and limited pediatric oncology surveillance capacity, all of which continue to complicate the accurate estimation of the true burden of childhood cancers across African settings.
|
Author/Year |
Country/Region |
Study Design |
Major Focus |
Key Findings |
|
Steliarova-Foucher et al. (2017) |
Global including Africa |
Population-based registry study |
International childhood cancer incidence |
Demonstrated geographic variation and surveillance limitations in LMICs |
|
Stoeter et al. (2021) [30] |
Uganda and Zimbabwe |
Registry-based study |
Childhood cancer incidence trends |
Reported changing incidence patterns over 25 years |
|
Kruger et al. (2014) [11] |
Africa |
Review article |
Childhood cancer epidemiology |
Summarized pediatric cancer burden across Africa |
|
Stefan et al. (2017) [12] |
Sub-Saharan Africa |
Review article |
Childhood cancer patterns |
Highlighted epidemiological distribution and healthcare disparities |
|
Bukirwa et al. (2020) [6] |
Uganda |
Registry study |
Cancer incidence trends |
Reported long-term changes in cancer incidence |
|
Chokunonga et al. (2013) [31] |
Zimbabwe |
Registry study |
Cancer incidence trends |
Identified temporal increases in reported cancers |
|
Owusu et al. (2023) [8] |
Ghana |
Retrospective observational study |
Childhood cancer incidence |
Described incidence patterns in tertiary hospitals |
|
Slone et al. (2014) [19] |
Zambia |
Retrospective cohort study |
Treatment outcomes |
Reported treatment abandonment challenges |
|
Davidson et al. (2014) [13] |
South Africa |
Observational study |
HIV-associated malignancies |
Linked HIV infection with pediatric malignancies |
|
Bohlius et al. (2016) [14] |
South Africa |
Record linkage study |
HIV-related cancers |
Examined incidence of AIDS-defining cancers |
|
Hämmerl et al. (2019) [38] |
Africa |
Review article |
Burkitt lymphoma burden |
Summarized epidemiology of endemic Burkitt lymphoma |
|
et al. (2008) [17] |
Uganda |
Epidemiological study |
Burkitt lymphoma distribution |
Linked malaria endemicity with Burkitt lymphoma |
|
Kotepui and Kotepui (2021) [16] |
Africa |
Systematic review and meta-analysis |
Malaria and Burkitt lymphoma |
Confirmed malaria-associated lymphoma risk |
|
Cunningham et al. (2020) |
Global including Africa |
Review article |
Wilms tumor disparities |
Reported major survival inequities |
|
Yun et al. (2011) |
Global |
Review article |
Retinoblastoma epidemiology |
Discussed epidemiology and RB1 genetics |
|
Gakunga and Parkin (2015) [24] |
Africa |
Survey study |
Cancer registry systems |
Evaluated operational capacity of registries |
|
Jedy-Agba et al. (2015) |
Nigeria |
Program report |
National cancer registration |
Described registry development efforts |
|
Parkin et al. (2021) [10] |
Sub-Saharan Africa |
Registry study |
Stage at diagnosis and survival |
Examined staging and survival patterns |
|
Mallon et al. (2023) [29] |
Sub-Saharan Africa |
Multicenter study |
Pediatric cancer staging |
Assessed feasibility of Toronto staging guidelines |
|
Ortiz et al. (2023) [27] |
Global including Africa |
Programmatic review |
WHO childhood cancer initiative |
Discussed pediatric oncology strengthening efforts |
Table 1: Representative Characteristics of Selected Included Studies
The geographic distribution of included studies demonstrated substantial regional variation in pediatric cancer research and surveillance coverage across Africa. Most studies originated from countries with relatively established cancer registries or pediatric oncology centers, including Uganda, Zimbabwe, South Africa, Ghana, Kenya, and Malawi, whereas several Central, North, and parts of West African countries remained underrepresented within the literature. Figure 2 illustrates the regional distribution of included studies and the concentration of pediatric cancer registry capacity across the continent.
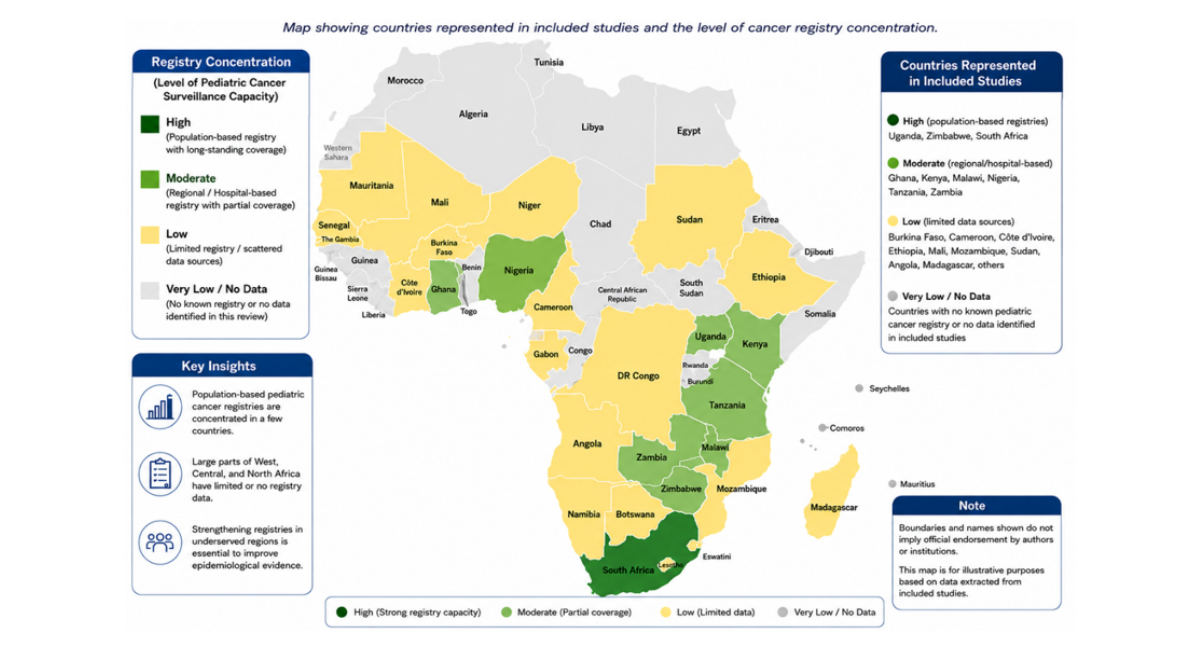
Figure 2: Regional Distribution of Included Studies and Pediatric Cancer Registries in Africa
The included studies demonstrated considerable geographic variation in the epidemiology and incidence patterns of pediatric cancer across Africa. Most studies reported increasing or increasingly recognized incidence trends over time, although substantial heterogeneity existed between countries, cancer types, and registry systems. Evidence from population-based cancer registries in Uganda, Zimbabwe, Malawi, Ghana, and South Africa suggested that improvements in cancer registration, diagnostic capacity, and pediatric oncology services contributed partly to the observed rise in reported childhood cancer incidence [7,8,30].
Leukemia, lymphoma, Wilms tumor, retinoblastoma, Kaposi sarcoma, and Burkitt lymphoma are the most frequently reported pediatric malignancies across the continent. Several studies have identified Burkitt lymphoma as one of the dominant childhood cancers in malaria-endemic regions of sub-Saharan Africa, particularly in Uganda, Ghana, Malawi, and parts of East and Central Africa [17]. The distribution of Burkitt lymphoma showed strong ecological associations with chronic malaria exposure and Epstein-Barr virus endemicity. Similarly, Kaposi sarcoma remains strongly associated with HIV prevalence and immunosuppression in several southern and eastern African countries [14].
Several registry-based studies have reported increasing incidence patterns for leukemias and solid tumors, particularly retinoblastoma and Wilms tumor, which may reflect both true epidemiological transitions and improved diagnostic recognition [6,31]. In contrast, underdiagnosis and underreporting remain persistent concerns in rural and resource-limited settings where pathology services and imaging infrastructure are limited. Multiple studies have emphasized that the true burden of pediatric cancers in Africa is likely substantially underestimated because of weak surveillance systems, incomplete cancer registration, treatment abandonment, and delayed healthcare-seeking behaviors [25,32].
Geographic disparities in pediatric cancer distribution have been consistently reported. Studies from West Africa frequently highlight Burkitt lymphoma, retinoblastoma, and nephroblastoma as dominant childhood malignancies, whereas southern African studies have more commonly reported HIV-associated cancers and leukemias [3,11]. North African studies have demonstrated a relatively higher reporting of central nervous system tumors and leukemias, potentially reflecting stronger diagnostic and neuroimaging capacity compared with many sub-Saharan settings.
Socioeconomic and health system factors substantially influence cancer incidence recognition and treatment outcomes. Delayed diagnosis, limited awareness, financial barriers, poor referral pathways, and shortages of pediatric oncology specialists have been repeatedly identified as contributors to advanced-stage presentation and poor survival outcomes [18,19]. Evidence from Ghana, Kenya, Zambia, and Burkina Faso further highlighted the impact of treatment abandonment, inadequate access to essential cancer medicines, and weak pediatric oncology infrastructure on continuity of care and survival [20,22,28].
The reviewed literature also demonstrated major disparities in cancer surveillance and registry quality across African nations. While some countries maintained long-standing population-based cancer registries with relatively robust reporting systems, several regions lacked functional pediatric cancer surveillance altogether [24]. Many studies emphasized incomplete case ascertainment, diagnostic inaccuracies, and inconsistent application of international childhood cancer classification systems as major barriers to reliable epidemiological comparisons [5,32]. Table 2 summarizes representative findings on incidence patterns, dominant cancer types, and major epidemiological observations reported across selected African studies.
|
Author/Year |
Country/Region |
Key Findings |
|
Stoeter et al. (2021) [30] |
Uganda & Zimbabwe |
Reported increasing childhood cancer incidence trends over 25 years with regional variation in cancer patterns |
|
Owusu et al. (2023) [8] |
Ghana |
Leukemias, lymphomas, nephroblastoma, and retinoblastoma were among the most frequently diagnosed childhood cancers |
|
Chasimpha et al. (2017) [7] |
Malawi |
Registry-based data demonstrated increasing cancer detection and persistent diagnostic limitations |
|
Ogwang et al. (2008) [32] |
Uganda |
Burkitt lymphoma distribution strongly correlated with malaria endemicity |
|
Hämmerl et al. (2019) |
Sub-Saharan Africa |
Highlighted the substantial burden of Burkitt lymphoma across malaria-endemic African regions |
|
Bohlius et al. (2016) [14] |
South Africa |
HIV-positive children demonstrated increased incidence of Kaposi sarcoma and other malignancies |
|
Kruger et al. (2014) [11] |
Africa |
Identified major disparities in pediatric oncology services and cancer outcomes across African countries |
|
Stefan (2015) [36] |
Africa |
Reported heterogeneous distribution of childhood cancers across African regions |
|
Bukirwa et al. (2020) [6] |
Uganda |
Demonstrated changing cancer incidence patterns and expanding registry reporting |
|
Parkin & Bray (2009) [25] |
Africa/Global |
Emphasized persistent incompleteness and quality limitations in cancer registry data |
|
Gakunga & Parkin (2015) [24] |
Africa |
Documented major disparities in operational cancer registry capacity across African countries |
|
Gupta et al. (2013) [20] |
LMICs including Africa |
Treatment abandonment emerged as a major contributor to poor pediatric cancer outcomes |
Table 2: Representative epidemiological findings and incidence patterns of pediatric cancers in Africa
Risk Factors and Determinants of Pediatric Cancers in Africa
The reviewed studies identified multiple biological, infectious, environmental, socioeconomic, and health system-related factors influencing the epidemiology and outcomes of pediatric cancers across Africa. Infectious diseases emerged as some of the most significant contributors to the distinct pediatric cancer landscape observed in many African settings. Several studies have demonstrated strong associations between Epstein-Barr Virus (EBV), malaria endemicity, and Burkitt lymphoma incidence, particularly in East and Central Africa [16,32,33]. Chronic exposure to Plasmodium falciparum infection has been repeatedly implicated in the pathogenesis and geographic clustering of endemic Burkitt lymphoma.
Human Immunodeficiency Virus (HIV) infection also plays a major role in pediatric cancer epidemiology across several African countries. Studies from South Africa, Uganda, and Zambia have reported an increased incidence of Kaposi sarcoma, lymphomas, and other malignancies among HIV-positive children [13,14]. Kaposi Sarcoma-Associated Herpesvirus (KSHV) seropositivity has been additionally linked with malaria co-infection and other parasitic infections in endemic communities, suggesting complex interactions between infectious diseases and cancer susceptibility.
Beyond infectious etiologies, several studies have highlighted the role of socioeconomic inequalities and structural determinants in shaping pediatric cancer outcomes across Africa. Poverty, financial hardship, weak referral systems, transportation barriers, and limited healthcare access contribute substantially to delayed diagnosis and treatment interruption [20,22]. Caregiver health literacy and awareness are consistently identified as important determinants of early healthcare-seeking behavior and treatment adherence [23,34].
Health system limitations represented another major determinant of poor pediatric cancer outcomes. Multiple studies have documented shortages of pediatric oncologists, pathologists, oncology nurses, radiotherapy facilities, and essential cancer medicines in many African countries [2,4] . Inadequate pathology infrastructure and delayed histopathological diagnosis frequently resulted in late-stage presentation and compromised treatment outcomes [35]. Several studies have reported that treatment abandonment remains a major challenge in resource-constrained settings due to financial constraints, prolonged treatment duration, sociocultural beliefs, and limited social support systems [19,22].
Environmental and demographic factors were less consistently reported but were identified in some studies. Geographic differences in malaria transmission intensity, urbanization patterns, and environmental exposure appear to influence regional variations in childhood cancer incidence [32]. Some studies have also suggested possible associations between socioeconomic deprivation and poorer survival outcomes among children with cancer.
Importantly, several studies have emphasized that many pediatric cancer risk factors in Africa remain insufficiently understood because of limited epidemiological research capacity, weak surveillance systems, and inadequate molecular diagnostic infrastructure. Consequently, substantial gaps persist regarding the contribution of genetic susceptibility, environmental carcinogens, and emerging epidemiological transitions to pediatric cancer patterns across the continent. Table 3 summarizes the major risk factors and determinants identified across the included studies.
|
Risk Factor/Determinant |
Associated Findings |
Representative Studies |
|
Malaria endemicity |
Strong association with Burkitt lymphoma incidence and geographic clustering |
|
|
Epstein–Barr virus (EBV) |
Implicated in endemic Burkitt lymphoma pathogenesis |
|
|
HIV infection |
Increased risk of Kaposi sarcoma and lymphomas |
Davidson et al. (2014); Bohlius et al. (2016) [14] |
|
KSHV infection |
Associated with Kaposi sarcoma and parasitic co-infections |
Nalwoga et al. (2018); Nalwoga et al. (2019) |
|
Poverty and financial hardship |
Contributed to delayed diagnosis and treatment abandonment |
Bekui et al. (2023); Gupta et al. (2014) [22] |
|
Weak referral systems |
Delayed specialist evaluation and advanced-stage presentation |
G et al. (2021); Slone et al. (2014) [21] |
|
Limited pathology infrastructure |
Reduced diagnostic accuracy and underreporting |
|
|
Shortage of oncology workforce |
Restricted access to specialized pediatric cancer care |
Stefan (2015); Srivastava et al. (2020) |
|
Poor caregiver health literacy |
Influenced healthcare-seeking behavior and treatment adherence |
|
|
Treatment abandonment |
Major contributor to poor survival outcomes |
Gupta et al. (2013); Kabore (2022) [20] |
Table 3: Major risk factors and determinants associated with pediatric cancers in Africa
Cancer Surveillance, Diagnostic Capacity, and Health System Challenges
The reviewed literature consistently identified major deficiencies in cancer surveillance systems, diagnostic infrastructure, and pediatric oncology capacity in many African countries. Weak population-based cancer registration systems, incomplete case ascertainment, inadequate pathology services, and limited pediatric oncology resources have been repeatedly reported as major barriers to accurately estimating the burden of pediatric cancers and improving treatment outcomes [24,25].
Several studies have emphasized that many African countries lack functional or nationally representative pediatric cancer registries. Existing registries are frequently concentrated in major urban centers and tertiary hospitals, thereby limiting the representativeness of national incidence estimates [7,30]. In addition, inconsistencies in reporting systems, incomplete follow-up data, and variations in the application of international childhood cancer classification systems complicate regional comparisons and trend analyses [5].
Diagnostic limitations emerged as a major challenge throughout the reviewed studies. Limited access to pathology services, immunohistochemistry, molecular diagnostics, neuroimaging, and radiologic infrastructure contributed to delayed or inaccurate diagnoses in many settings [35] Louis et al., 2016). Several studies have reported that children frequently present with advanced-stage disease because of prolonged diagnostic delays and weak referral pathways [18]. In some rural and low-resource settings, misclassification and underdiagnosis of pediatric malignancies remain substantial concerns, particularly for leukemias and central nervous system tumors.
Workforce shortages further constrained pediatric oncology care across the continent. Multiple studies have documented insufficient numbers of pediatric oncologists, oncology nurses, pathologists, radiologists, and supportive care specialists in many African countries [36]. These workforce gaps limited access to timely diagnosis, treatment initiation, supportive care, and long-term follow-up services. The uneven distribution of specialized oncology centers also created major geographic disparities in access to care, particularly for rural populations.
Access to essential cancer medicines and treatment infrastructure is another major challenge identified in the literature. Studies from East, West, and Southern Africa have highlighted recurrent shortages of chemotherapy agents, radiotherapy services, blood products, and supportive care medications [4,28]. Financial hardship, transportation costs, and prolonged treatment schedules frequently contribute to treatment interruption and abandonment, particularly among low-income households [20,22].
Several studies have nevertheless reported emerging progress in pediatric cancer control efforts across Africa. The expansion of cancer registries, strengthening of pediatric oncology units, regional collaborations, implementation of treatment guidelines, and participation in the WHO Global Initiative for Childhood Cancer were identified as important advances in selected countries [27,29]. Efforts to improve early detection, workforce development, access to essential medicines, and standardized staging systems are increasingly being integrated into national cancer control strategies.
Despite these improvements, the reviewed evidence demonstrates persistent disparities in pediatric oncology infrastructure and surveillance capacity across African regions. The literature consistently emphasizes that strengthening cancer registration systems, diagnostic services, pathology infrastructure, oncology workforce capacity, and equitable access to treatment is essential for improving pediatric cancer outcomes and generating more reliable epidemiological data across Africa as summarised in Table 4.
|
Challenge Area |
Key Issues Identified |
Representative Studies |
|
Cancer registration systems |
Incomplete case ascertainment, urban-centered registries, inconsistent reporting |
|
|
Data quality limitations |
Underreporting, missing follow-up data, classification inconsistencies |
Parkin & Bray (2009) [25]; Steliarova-Foucher et al. (2024) |
|
Diagnostic infrastructure |
Limited pathology services, imaging shortages, delayed diagnosis |
Naresh et al. (2011) [35]; Louis et al. (2016) |
|
Advanced-stage presentation |
Delayed healthcare-seeking and weak referral systems |
Mullen et al. (2021); Slone et al. (2014) [21] |
|
Workforce shortages |
Insufficient pediatric oncologists, pathologists, oncology nurses |
Stefan (2015) [36]; Srivastava et al. (2020) |
|
Limited access to medicines |
Chemotherapy shortages and weak procurement systems |
Petricca et al. (2024); Renner et al. (2018) [28] |
|
Treatment abandonment |
Financial barriers and prolonged treatment duration |
|
|
Geographic disparities |
Unequal distribution of oncology services and specialized centers |
Kruger et al. (2014); Stefan et al. (2017) [12] |
|
Emerging system improvements |
Expansion of registries, WHO initiatives, regional collaborations |
Table 4: Major surveillance, diagnostic, and health system challenges identified across included studies
Implications for Pediatric Cancer Prevention and Control in Africa
The findings of this scoping review highlight major implications for pediatric cancer prevention, early detection, surveillance strengthening, treatment access, and health system development across Africa. Although pediatric cancers are increasingly recognized across the continent, substantial inequities persist in access to diagnosis, treatment, supportive care, and survivorship services. These disparities continue to contribute to poor treatment outcomes and low survival rates in many African settings despite significant advances in pediatric oncology globally.
Strengthening pediatric cancer surveillance systems emerged as one of the most critical priorities identified across the reviewed literature. Multiple studies have reported that weak population-based cancer registries, incomplete reporting systems, limited pathology infrastructure, and poor mortality surveillance continue to obscure the true burden of pediatric cancers across Africa [24,25]. Therefore, strengthening and expanding pediatric cancer registration systems is essential for generating reliable epidemiological data, monitoring incidence trends, evaluating interventions, and informing evidence-based cancer control policies. The expansion of registry networks through initiatives such as the African Cancer Registry Network (AFCRN) may substantially improve regional surveillance capacity and facilitate more reliable continent-wide comparisons.
The reviewed evidence further underscores the importance of early detection and timely referral in improving pediatric cancer outcomes. Delayed presentation and advanced-stage disease have been consistently reported across multiple African settings and are frequently associated with poor survival outcomes and increased treatment-related mortality. Several studies have emphasized that low public awareness, weak referral pathways, shortages of trained healthcare workers, and limited diagnostic capacity continue to contribute to diagnostic delays. Community-based awareness campaigns, caregiver education programs, school health initiatives, and targeted training of frontline healthcare providers may therefore facilitate earlier recognition of childhood cancer warning signs and improve referral efficiency. Strengthening pathology, imaging, and laboratory services also remains essential for improving diagnostic accuracy and treatment planning.
The findings additionally highlight the importance of integrating pediatric cancer prevention and control strategies within broader public health and communicable disease programs. Strong associations between HIV, malaria, Epstein–Barr Virus (EBV), Kaposi Sarcoma-associated Herpesvirus (KSHV), and certain pediatric malignancies suggest that infectious disease prevention efforts may indirectly contribute to reducing the burden of infection-associated childhood cancers, such as Burkitt lymphoma and Kaposi sarcoma [14,18,32]. Expanded HIV prevention programs, antiretroviral therapy coverage, malaria control interventions, and strengthened infectious disease surveillance may therefore have important implications for pediatric cancer prevention in several African regions.
Health system strengthening emerged as another major priority across the reviewed studies. Persistent shortages of pediatric oncologists, oncology nurses, pathologists, radiologists, radiotherapy facilities, and essential cancer medicines continue to limit access to quality pediatric oncology care in many African countries [2,4]. Several studies emphasized the need to expand pediatric oncology workforce training, strengthen multidisciplinary care teams, improve referral coordination, and increase investment in specialized pediatric oncology centers. Regional training collaborations and partnerships with international pediatric oncology networks may further support workforce development and capacity strengthening in resource-constrained settings.
The reviewed literature also demonstrated that treatment interruption and abandonment remain major barriers to effective pediatric cancer control in Africa. Financial hardship, transportation costs, prolonged treatment schedules, inadequate accommodation near treatment centers, and weak psychosocial support systems have been identified as major contributors to poor treatment adherence [20,22]. Interventions aimed at reducing out-of-pocket costs, expanding national health insurance coverage, improving caregiver support systems, and strengthening social welfare programs may substantially improve treatment completion and survival outcomes. Access to affordable pediatric cancer medicines and supportive care services also remains a critical component of childhood cancer control efforts across Africa. Several studies have highlighted recurring shortages of chemotherapy agents, supportive medicines, blood products, and diagnostic supplies within many treatment centers [4]. Strengthening medicine procurement systems, regional supply chain coordination, and national financing mechanisms may therefore improve continuity of care and reduce preventable treatment-related mortality.
The findings of this review additionally reinforce the importance of the WHO Global Initiative for Childhood Cancer as a strategic framework for advancing pediatric oncology care across African settings. The initiative’s emphasis on early diagnosis, strengthened referral systems, access to essential medicines, improved cancer registration, and health system strengthening aligns closely with many of the gaps identified throughout the reviewed literature [26,27]. Sustained political commitment, increased domestic investment, and regional collaboration will be essential for translating these priorities into measurable improvements in childhood cancer survival across the continent. The review also identified important research gaps. Many African countries remain underrepresented in pediatric oncology research, and studies exploring genetic determinants, environmental exposures, survivorship outcomes, molecular epidemiology, and long-term treatment outcomes are limited in number. Therefore, increased investment in multi-country epidemiological studies, collaborative pediatric oncology research networks, and standardized data systems is essential for advancing evidence-based prevention and control strategies across Africa.
Collectively, the evidence synthesized in this scoping review demonstrates that improving pediatric cancer outcomes in Africa requires coordinated investments in surveillance systems, early detection initiatives, infectious disease control, workforce development, treatment infrastructure, medicine access, referral pathways, and context-specific research. Strengthening these interconnected areas will be critical for advancing pediatric cancer prevention and control efforts and supporting progress toward the goals of the WHO Global Initiative for Childhood Cancer across African settings.
DISCUSSION
This scoping review mapped and synthesized the available evidence on the epidemiology and emerging trends of pediatric cancers in Africa, with an emphasis on incidence patterns, geographic distribution, risk factors, surveillance limitations, and implications for prevention and control. The findings demonstrate that childhood cancers represent an increasingly important public health challenge across the continent, although the true burden remains incompletely characterized because of persistent deficiencies in cancer registration systems, diagnostic infrastructure, pathology services, and epidemiological surveillance capacity.
The reviewed studies consistently demonstrated increasing or increasingly recognized incidence patterns of pediatric cancers across several African countries over recent decades. Registry-based studies from Uganda, Zimbabwe, Malawi, Ghana, and South Africa reported rising incidence trends for leukemias, lymphomas, Wilms tumor, retinoblastoma, and Kaposi sarcoma [6,8,30]. Similar patterns have been documented globally, where international surveillance studies have reported increasing incidence rates for several childhood malignancies over time [5,9]. However, interpretation of these patterns within African contexts requires caution. In many settings, increasing incidence may partly reflect improvements in diagnostic capacity, expansion of cancer registration systems, improved pathology services, and greater clinical recognition of childhood malignancies rather than true increases in disease occurrence alone. Nevertheless, the findings strongly suggest that pediatric cancers are becoming increasingly visible within African health systems and require greater policy and public health attention.
The review further demonstrated marked geographic variation in pediatric cancer patterns across the continent. Burkitt lymphoma and Kaposi sarcoma were more frequently reported in malaria-endemic and HIV-prevalent regions of sub-Saharan Africa, whereas leukemias and solid tumors appeared increasingly recognized in urbanized settings with relatively stronger diagnostic infrastructure and oncology services. These findings reinforce the important role of infectious, environmental, and socioeconomic determinants in shaping childhood cancer epidemiology within African settings. The observed associations between Epstein-Barr Virus (EBV), malaria, HIV infection, and specific pediatric malignancies remain consistent with earlier evidence linking chronic infectious exposures and immunosuppression to the development of Burkitt lymphoma and Kaposi sarcoma [14,16,32]. The persistence of infection-associated malignancies across several African regions further highlights the interconnected nature of communicable diseases and pediatric oncology within many LMIC contexts. Beyond infectious determinants, the findings highlighted the major influence of structural and socioeconomic factors on pediatric cancer outcomes across Africa. Delayed diagnosis, treatment abandonment, weak referral pathways, limited pathology services, financial hardship, shortages of pediatric oncology specialists, and inconsistent access to cancer medicines were repeatedly identified across the reviewed studies [21,22]. In many African settings, children continue to present with advanced-stage disease, thereby reducing treatment effectiveness and survival probabilities. These findings align with broader global pediatric oncology literature demonstrating that survival disparities between high-income countries and LMICs are driven not only by disease biology but also by profound inequities in health system capacity, healthcare access, and supportive care infrastructure [37].
One of the most important findings of this review relates to persistent weaknesses in pediatric cancer surveillance systems across Africa. The reviewed literature consistently emphasizes that incomplete population-based cancer registration inconsistent reporting systems, underdeveloped pathology services, and limited mortality surveillance continue to obscure the true burden of pediatric cancers across many African countries [24,25]. Many countries remain underrepresented in global childhood cancer datasets, and available registry data are often restricted to urban centers and tertiary institutions. Consequently, regional comparisons remain difficult, and current incidence estimates likely underestimate the actual magnitude of the disease burden. These surveillance limitations represent a major obstacle to effective pediatric cancer planning, resource allocation, service expansion, and evidence-based policy development across the continent.
The findings of this review also underscore the importance of strengthening integrated pediatric cancer prevention and control strategies within African settings. Infection-associated malignancies, such as Burkitt lymphoma and Kaposi sarcoma, highlight the potential indirect benefits of malaria control programs, HIV prevention initiatives, expanded antiretroviral therapy coverage, and strengthened infectious disease surveillance systems. At the same time, improving childhood cancer outcomes will require coordinated investments in early detection programs, community awareness initiatives, pathology infrastructure, referral systems, pediatric oncology workforce training, and equitable access to essential medicines and supportive care services. The WHO Global Initiative for Childhood Cancer provides an important strategic framework for advancing these priorities through strengthened health systems, improved cancer registration, expanded access to treatment, and workforce capacity development [26,27].
To further contextualize the interconnected determinants, health system challenges, and intervention priorities influencing pediatric cancer outcomes across African settings, a conceptual framework illustrating the major drivers and control pathways identified in this review is presented in Figure 2.
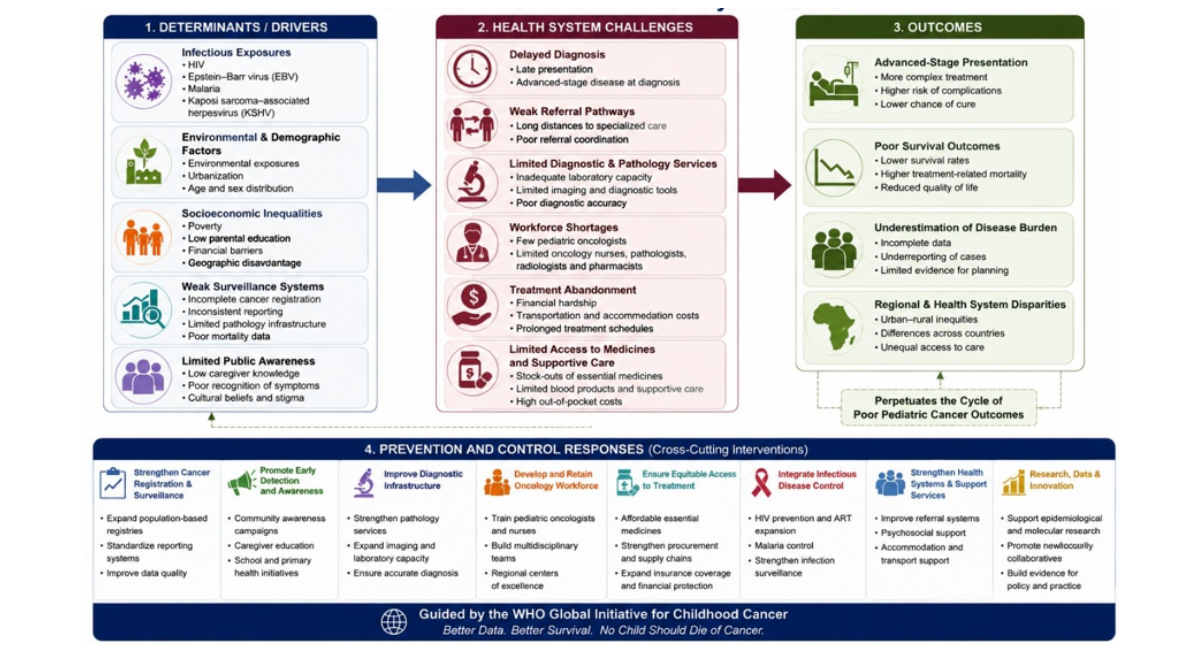
Figure 3: Conceptual Framework of Determinants and Pediatric Cancer Prevention and Control Pathways in Africa
This review also identified substantial research gaps in the literature on African pediatric oncology. Several African regions remain poorly represented in published studies, and longitudinal incidence analyses, molecular epidemiological studies, survivorship research, genomic investigations, and multicountry collaborative analyses are limited. Furthermore, evidence regarding environmental risk factors, long-term treatment outcomes, psychosocial impacts, and survivorship care remains insufficient in Africa. Increased investment in standardized population-based registries, multicountry pediatric oncology collaborations, and context-specific epidemiological research is essential for generating more accurate evidence to guide future prevention and control strategies in this field.
The findings of this review should be interpreted alongside certain limitations. The included studies varied substantially in design, registry coverage, methodological quality, diagnostic approaches, and reporting standards, thereby limiting direct comparability across settings. Underreporting, incomplete case ascertainment, and diagnostic limitations may additionally have contributed to the underestimation of disease burden in several countries. Moreover, substantial heterogeneity in registry infrastructure and healthcare access across African settings may have influenced observed incidence patterns and geographic comparisons. Nevertheless, this scoping review provides one of the most comprehensive syntheses to date of the evolving epidemiological landscape of pediatric cancers in Africa and highlights critical priorities for surveillance strengthening, early detection, research, and pediatric cancer control across the continent.
Implications for Pediatric Cancer Prevention and Control in Africa
The findings of this scoping review have important implications for pediatric cancer prevention, surveillance, clinical management, and health system strengthening across Africa. The growing recognition of childhood cancers on the continent underscores the urgent need for coordinated and context-specific interventions aimed at improving early diagnosis, expanding access to quality care, and strengthening pediatric oncology systems.
One of the most critical priorities identified across the reviewed literature is the strengthening of cancer surveillance systems and population-based cancer registries. Reliable epidemiological data remain essential for understanding coverage, data completeness, pathology reporting, and mortality surveillance [24,25]. Therefore, expanding and strengthening population-based pediatric cancer registries, particularly in underserved and rural settings, will be fundamental for improving childhood cancer control efforts across the disease burden, monitoring incidence trends, informing policy decisions, and guiding resource allocation. However, many African countries continue to experience substantial gaps in cancer registration continent.
This review also highlights the need to strengthen early detection and referral systems. Delayed diagnosis remains a major contributor to poor survival outcomes in many African settings, often resulting from limited public awareness, weak referral pathways, inadequate pathology services, and a shortage of trained healthcare professionals [21]. Integrating childhood cancer awareness into primary healthcare systems, school health programs, maternal and child health services, and community health initiatives may contribute to the earlier recognition of warning signs and more timely referral of affected children.
Workforce development emerged as another major priority. Several studies have emphasized the persistent shortages of pediatric oncologists, oncology nurses, pathologists, radiologists, and specialized laboratory personnel across African countries [36,37]. Expanding oncology training programs, strengthening multidisciplinary pediatric cancer teams, and supporting regional centers of excellence may help improve diagnostic accuracy, treatment delivery, and long-term patient outcomes. Regional and international partnerships may further support workforce capacity building, mentorship, and collaborative research initiatives.
These findings reinforce the importance of improving equitable access to pediatric cancer medicines, diagnostics, and supportive care services. Financial hardship, treatment interruption, medicine shortages, and treatment abandonment remain major barriers to effective childhood cancer management in many African countries [19,22]. Strengthening national procurement systems, expanding health insurance coverage, improving supply chain management, and integrating childhood cancer treatment into universal health coverage frameworks may improve treatment continuity and survival outcomes.
Given the important contribution of infectious diseases to the pediatric cancer landscape in Africa, integrated approaches linking infectious disease control with pediatric oncology programs may also provide important public health benefits. HIV control programs, malaria prevention strategies, expanded antiretroviral therapy coverage, and improved infection surveillance may indirectly contribute to reductions in infection-associated childhood malignancies, such as Burkitt lymphoma and Kaposi sarcoma [14,38]. These findings highlight the importance of adopting multisectoral and integrated health system approaches to pediatric cancer prevention and control within African contexts.
The WHO Global Initiative for Childhood Cancer provides an important framework for advancing many of these priorities through strengthened health systems, improved access to essential medicines, enhanced cancer registration, and expanded pediatric oncology services [26,27]. Sustained political commitment, increased domestic investment, regional collaboration, and context-specific research are essential for translating these initiatives into measurable improvements in childhood cancer outcomes across Africa.
CONCLUSION
Pediatric cancer is an increasingly important public health and health system challenge across Africa. The evidence synthesized in this scoping review indicates that childhood malignancies, including leukemias, lymphomas, Wilms tumor, retinoblastoma, Kaposi sarcoma, and Burkitt lymphoma, are increasingly recognized across several African settings, although substantial geographic and epidemiological variations persist. Infectious exposures, such as HIV, Epstein–Barr virus, malaria, and Kaposi sarcoma-associated herpesvirus, continue to play a major role in shaping pediatric cancer patterns within many sub-Saharan African regions.
The findings of this review demonstrate that the true burden of pediatric cancer across Africa remains incompletely characterized because of persistent weaknesses in population-based cancer registration systems, pathology infrastructure, diagnostic services, and epidemiological surveillance. Delayed diagnosis, treatment abandonment, shortages of pediatric oncology specialists, limited access to essential medicines, and major socioeconomic barriers continue to contribute to poor survival outcomes across many African countries. These challenges remain particularly pronounced in low-resource and underserved settings where specialized pediatric oncology services are limited or absent.
At the same time, the reviewed evidence reflects increasing momentum toward strengthening pediatric cancer control efforts across the continent. The expansion of cancer registries, growing regional research collaborations, strengthening of pediatric oncology units, and implementation of the WHO Global Initiative for Childhood Cancer represent important advances toward improving childhood cancer outcomes in African settings. Nevertheless, major gaps remain in longitudinal surveillance data, survivorship research, molecular epidemiology, genomic studies, and multicountry collaborative evidence.
The findings of this scoping review underscore the urgent need for coordinated and sustained investments in the prevention and control of pediatric cancer across Africa. Strengthening population-based cancer registries, expanding diagnostic and pathology capacity, improving early detection systems, increasing access to affordable treatment, strengthening pediatric oncology workforce development, and integrating childhood cancer priorities within broader public health frameworks are essential for improving survival outcomes and reducing disparities in pediatric cancer care across the continent. Future progress will require strong political commitment, increased domestic and international investment, regional collaboration, and context-specific pediatric oncology research capable of informing evidence-based interventions and policy development. Advancing these priorities will be critical for strengthening pediatric oncology systems in Africa and supporting global efforts to improve the survival and quality of life of children affected by cancer.
ABBREVIATIONS
AFCRN = African Cancer Registry Network; ART = Antiretroviral Therapy; EBV = Epstein–Barr Virus; HIV = Human Immunodeficiency Virus; IARC = International Agency for Research on Cancer; KSHV = Kaposi Sarcoma-Associated Herpesvirus; LMICs = Low- And Middle-Income Countries; WHO = World Health Organization.
REFERENCES
- Ward E, DeSantis C, Robbins A, Kohler B, Jemal A. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin. 2014 Mar;64(2):83-103. [Crossref] [Google Scholar] [PubMed]
- Siegel DA, Richardson LC, Henley SJ, Wilson RJ, Dowling NF, Weir HK, et al. Pediatric cancer mortality and survival in the United States, 2001–2016. Cancer. 2020;126(19):4379-4389. [Crossref] [Google Scholar] [PubMed]
- Stefan DC. Childhood cancer in Africa: an overview of resources. J Pediatr Hematol Oncol. 2015;37(2):104-108. [Crossref] [Google Scholar] [PubMed]
- Petricca K, Carson L, Kambugu J, Denburg A. Strengthening access to cancer medicines for children in East Africa: policy options to enhance medicine procurement, forecasting, and regulations. Glob Health Res Policy. 2024 ;9(1):24. [Crossref] [Google Scholar] [PubMed]
- Steliarova-Foucher E, Colombet M, Ries LA, Moreno F, Dolya A, Bray F, et al. International incidence of childhood cancer, 2001–10: a population-based registry study. Lancet Oncol. 2017;18(6):719-731. [Crossref] [Google Scholar] [PubMed]
- Bukirwa P, Wabinga H, Nambooze S, Amulen PM, Joko WY, Liu B, Parkin DM. Trends in the incidence of cancer in Kampala, Uganda, 1991 to 2015. Int J Cancer. 2021;148(9):2129-1238. [Crossref] [Google Scholar] [PubMed]
- Chasimpha SJ, Parkin DM, Masamba L, Dzamalala CP. Three‐year cancer incidence in Blantyre, Malawi (2008–2010). Int J Cancer. 2017;141(4):694-700. [Crossref] [Google Scholar] [PubMed]
- Owusu WE, Burger JR, Lubbe MS, Joubert R, Cockeran M. Incidence patterns of childhood cancer in two tertiary hospitals in Ghana from 2015 to 2019: a retrospective observational study. Cancer Epidemiol. 2023;87:102470. [Crossref] [Google Scholar] [PubMed]
- Zhao Y, Sun P, Xiao J, Jin L, Ma N, Li Z, et al. International patterns and trends of childhood and adolescent cancer, 1978-2012. J Natl Cancer Cent. 2022;2(2):78-89. [Crossref] [Google Scholar] [PubMed]
- Parkin DM, Youlden DR, Chitsike I, Chokunonga E, Couitchéré L, Gnahatin F, et al. Stage at diagnosis and survival by stage for the leading childhood cancers in three populations of sub‐Saharan Africa. Int J Cancer. 2021;148(11):2685-91. [Crossref] [Google Scholar] [PubMed]
- Kruger M, Hendricks M, Davidson A, Stefan CD, van Eyssen AL, Uys R, van Zyl A, Hesseling P. Childhood cancer in Africa. Pediatr Blood Cancer. 2014;61(4):587-592. [Crossref] [Google Scholar] [PubMed]
- Stefan C, Bray F, Ferlay J, Liu B, Parkin DM. Cancer of childhood in sub-Saharan Africa. Ecancermedicalscience. 2017;11:755. [Crossref] [Google Scholar] [PubMed]
- Davidson A, Wainwright RD, Stones DK, Kruger M, Hendricks M, Geel J, et al. Malignancies in South African children with HIV. J Pediatr Hematol Oncol. 2014;36(2):111-117. [Crossref] [Google Scholar] [PubMed]
- Bohlius J, Maxwell N, Spoerri A, Wainwright R, Sawry S, Poole J, et al. Incidence of AIDS-defining and other cancers in HIV-positive children in South Africa: record linkage study. Pediatr Infect Dis J. 2016;35(6):e164-70. [Crossref] [Google Scholar] [PubMed]
- Ogwang MD, Bhatia K, Biggar RJ, Mbulaiteye SM. Incidence and geographic distribution of endemic Burkitt lymphoma in northern Uganda revisited. International journal of cancer. 2008;123(11):2658-2663. [Crossref] [Google Scholar] [PubMed]
- Hämmerl L, Colombet M, Rochford R, Ogwang DM, Parkin DM. The burden of Burkitt lymphoma in Africa. Infectious agents and cancer. 2019;14(1):17. [Crossref] [Google Scholar] [PubMed]
- Kotepui KU, Kotepui M. Malaria infection and risk for endemic Burkitt lymphoma: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(11):5886. [Crossref] [Google Scholar] [PubMed]
- Slone JS, Chunda-Liyoka C, Perez M, Mutalima N, Newton R, Chintu C, et al. Pediatric malignancies, treatment outcomes and abandonment of pediatric cancer treatment in Zambia. PloS one. 2014;9(2):e89102. [Crossref] [Google Scholar] [PubMed]
- Gupta S, Yeh S, Martiniuk A, Lam CG, Chen HY, Liu YL, et al. The magnitude and predictors of abandonment of therapy in paediatric acute leukaemia in middle-income countries: a systematic review and meta-analysis. Eur J Cancer. 2013;49(11):2555-2564. [Crossref] [Google Scholar] [PubMed]
- Mullen CJ, Barr RD, Franco EL. Timeliness of diagnosis and treatment: the challenge of childhood cancers. Br J Cancer. 2021;125(12):1612-1620. [Crossref] [Google Scholar] [PubMed]
- Bekui BA, Ohene LA, Badzi C, Ampomah MO, Aziato L. Physical and socioeconomic burden of caregiving on family caregivers of children with cancer at a tertiary Hospital in Ghana. Nurs Open. 2023;10(2):915-25. [Crossref] [Google Scholar] [PubMed]
- Nurhidayah I, Hendriyani D, Adistie F, Nurhaeni N, Mediani HS. Factors influencing treatment-seeking behavior among caregivers of children with cancer: a scoping review. J Multidiscip Healthc. 2025:563-578. [Crossref] [Google Scholar] [PubMed]
- Gakunga R, Parkin DM, African Cancer Registry Network. Cancer registries in Africa 2014: A survey of operational features and uses in cancer control planning. Int J Cancer. 2015;137(9):2045-2052. [Crossref] [Google Scholar] [PubMed]
- Parkin DM, Bray F. Evaluation of data quality in the cancer registry: principles and methods Part II. Completeness. Eur J Cancer. 2009;45(5):756-764. [Crossref] [Google Scholar] [PubMed]
- World Health Organization. Global initiative for childhood cancer: an overview. 2021.
- Ortiz R, Vásquez L, Giri B, Kapambwe S, Dille I, Mahmoud L, et al. Developing and sustaining high-quality care for children with cancer: the WHO Global Initiative for Childhood Cancer. Rev Panam Salud Publica. 2024;47:e164. [Crossref] [Google Scholar] [PubMed]
- Renner L, Shah S, Bhakta N, Denburg A, Horton S, Gupta S. Evidence from Ghana indicates that childhood cancer treatment in sub-Saharan Africa is very cost effective: a report from the childhood cancer 2030 network. J Glob Oncol. 2018;4:1-9. [Crossref] [Google Scholar] [PubMed]
- Mallon B, Kaboré R, Couitchere L, Akonde FB, Narison ML, Budiongo A, et al. The feasibility of implementing Toronto childhood cancer stage guidelines and estimating the impact on outcome for childhood cancers in seven pediatric oncology units in sub‐Saharan Africa. A study from the Franco‐African Pediatric Oncology Group. Pediatric Blood & Cancer. 2023;70(12):e30664. [Crossref] [Google Scholar] [PubMed]
- Stoeter O, Seraphin TP, Chitsike I, Chokunonga E, Kambugu JB, Wabinga H, et al. Trends in childhood cancer incidence in sub‐Saharan Africa: Results from 25 years of cancer registration in Harare (Zimbabwe) and Kyadondo (Uganda). Int J Cancer. 2021;149(5):1002-1012. [Crossref] [Google Scholar] [PubMed]
- Chokunonga E, Borok MZ, Chirenje ZM, Nyakabau AM, Parkin DM. Trends in the incidence of cancer in the black population of Harare, Zimbabwe 1991–2010. Int J Cancer. 2013;133(3):721-729. [Crossref] [Google Scholar] [PubMed]
- Ward ZJ, Yeh JM, Bhakta N, Frazier AL, Atun R. Estimating the total incidence of global childhood cancer: a simulation-based analysis. Lancet Oncol. 2019;20(4):483-493. [Crossref] [Google Scholar] [PubMed]
- Arisue N, Chagaluka G, Palacpac NM, Johnston T, Mutalima N, Peprah S, et al. Assessment of mixed Plasmodium falciparum sera5 infection in endemic Burkitt lymphoma: A case-control study in Malawi. Cancers. 13(7);1692. [Crossref] [Google Scholar] [PubMed]
- Moore C, Gallagher P, Dunne S. Health literacy, eHealth literacy and their association with burden, distress, and self-efficacy among cancer caregivers. Front Psychol. 2024;15:1283227.. [Crossref] [Google Scholar] [PubMed]
- Naresh KN, Raphael M, Ayers L, Hurwitz N, Calbi V, Rogena E, et al. Lymphomas in sub‐Saharan Africa–what can we learn and how can we help in improving diagnosis, managing patients and fostering translational research?. Br J Haematol. 2011 Sep;154(6):696-703. [Crossref] [Google Scholar] [PubMed]
- Magrath I, Epelman S. Cancer in adolescents and young adults in countries with limited resources. Current oncology reports. 2013 Aug;15(4):332-346. [Crossref] [Google Scholar] [PubMed]
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 25-35 Days |
Peer Review Feedback |
| 45-60 Days | Total article processing time |
Journal Flyer