Journal of Artificial Intelligence and Digital Health
ISSN:
3139-6267 (Online)
DOI Prefix (Crossref): 10.67238
ABSTRACT
The integration of Artificial Intelligence (AI), Big Data analytics, and the Internet of Things (IoT) is the key to the digital healthcare transformation in developing countries. This paper examines the combined effect of these technologies in improving digital healthcare in Bangladesh, a developing economy, which is typified by poor infrastructure and unequal distribution of health services. With the help of a quantitative, primary data-driven methodology, 385 respondents were selected based on healthcare systems, hospital managers, patients, and technology developers at Dhaka, Chittagong, Rajshahi, and Sylhet and administered the structured questionnaires. SPSS v.26 was used in the analysis of data, which included descriptive statistics, Pearson correlation, and multiple regression analysis. The results indicate that all three categories of AI-based diagnostic tools, IoT-based remote patient monitoring, and big data health analytics explain 73.4 per cent of the difference in the quality of digital health services (R2= 0.734, p = 0.001). Integration of IoT became the most powerful individual predictor (= 0.412), then there were AI application (= 0.381) and utilisation of big data = 0.297). The research has determined the infrastructure gaps, data privacy and poor levels of digital literacy as the major obstacles. The article makes a contribution to the theory of the Technology Acceptance Model (TAM) and a practical suggestion of a Bangladesh Digital Health Framework (BDHF) that can be utilised to make evidence-based policies.
Keywords: Artificial Intelligence; Big Data; Internet of Things; Digital Healthcare; Bangladesh; Emerging Economy; Health Informatics
INTRODUCTION
The healthcare situation in the world is experiencing a paradigm shift, as the fast development of Artificial Intelligence (AI), analytics with Big Data, and Internet of Things (IoT) influences the sphere. All of these digital health technologies transform the traditional healthcare delivery, monitoring, and management model, especially in environments with limited resources where traditional healthcare infrastructure is still in place [1-2]. In the case of emerging economies, the use of these technologies is not only an opportunity to pursue an incremental change, but it is also a platform through which they can realise Universal Health Coverage (UHC) and Sustainable Development Goal 3 (SDG 3).
Bangladesh (population over 170 million) is one of the examples of a country that is facing healthcare issues common to many other emerging economies: it has the number of specialists per 1,000 population of about 0.58, with the distribution of professionals being disproportionally concentrated in urban centres, and rural health access being highly unequal WHO, MOHFW, These structural vulnerabilities were additionally revealed during the COVID-19 pandemic and at the same time increased the rate of adoption of telemedicine and digital health innovations in the country [3-4]. The policy environment that has been established by government-led initiatives like the Digital Bangladesh Vision 2021 and its successor, Smart Bangladesh Vision 2041, has been conducive towards the integration of health-technology (Bangladesh Telecommunication Regulatory Commission [BTRC]) [5].
Although the current amount of literature on AI, Big Data, and IoT in healthcare is growing globally, there is limited empirical research on the topic within the South Asian and Bangladeshi healthcare setting, in particular. The available literature often focuses on rich countries with developed digital infrastructure, which makes their results of little use in developing economies [6-7]. In addition, no previous research by the Bangladeshi healthcare system has adequately focused on the simultaneous application of all three technologies, as the use of secondary data or qualitative research in the majority of such studies does not provide the opportunity to make a causal conclusion.
This paper fills these gaps through the analysis of the impact that the combined implementation of AI, Big Data, and IoT technologies has on the quality of digital healthcare and its accessibility in Bangladesh. The policy-makers, health care administrators, and developers of technology can use the research as an evidence-based source of actionable information using primary quantitative data and rigorous statistical analysis with the help of SPSS. The article is written in a systematic review of the appropriate literature, research methodology description, results and findings presentation, critical discussion, specific recommendations, and ends briefly with the conclusion.
LITERATURE REVIEW
Artificial Intelligence in Digital Healthcare
The field of artificial intelligence has become a game-changer in the clinical decision-making process, diagnostics and management of health systems. Computer vision applications, machine learning algorithms, and natural language processing (NLP) have proven to be very effective in the diagnosis of many diseases, including diabetic retinopathy and tuberculosis [8-9]. In low- and middle-income countries (LMICs), AI-assisted diagnostics has a specific potential, where the existing shortage of specialists in the field of physicians is filled in. Esteva were able to show that deep learning models were as accurate in categorising dermatological conditions as board-certified dermatologists, and this has a far-reaching implication on rural Bangladeshi societies that rely on primary care workers [10]. The same was reported by Jiang who reported AI ability in supporting clinical judgment in cancer diagnosis, and Obermeyer and Emanuel offered an early systematic review of the machine learning use in healthcare areas [11-12].
Big Data Analytics in Health Systems
Healthcare Big Data refers to the process of collecting, integrating and analysing heterogeneous health data (such as electronic health records (EHRs), genomic data, insurance claims, wearable sensor data and others) at a large scale to produce actionable clinical and operational insights [13]. In up-and-coming economies, large-scale data analytics can be used to facilitate epidemiological surveillance, optimisation of supply chains and resource allocation decisions that are essential in the administration of the population [14]. Shameer reported the increasing role of big data in personalised medicine, whereas Chen presented the background information on the business intelligence applications, which can be extended to health administration [15-16]. In the Bangladeshi case, the data repositories held by the Directorate General of Health Services (DGHS) can be used to a great effect to enhance the estimates of disease burden, vaccination coverage, and maternal mortality surveillance, should advanced analytics be used in harnessing such information [17].
Internet of Things in Medical Applications
Healthcare Internet of Things (also known as the Internet of Medical Things (IoMT)) is a network of medical devices, wearable devices, remote patient monitoring systems, and smart hospital infrastructure [18]. The telemonitoring, which is IoT-enabled, has been effective in chronic disease management, including hypertension, diabetes, and cardiac arrhythmias, because it allows real-time transmission of physiological data by patients to clinicians [19]. Bhatt and Bhatt highlighted the use of IoT in monitoring medication adherence, whereas Javaid listed the latest applications of the IoT in post-surgical care and monitoring of the elderly [7-20]. In the case of Bangladesh, the IoT infrastructure, specifically mobile health (mHealth) systems that are based on the widespread coverage of the mobile network (96 per cent penetration) in this nation, provides an opportunity to provide more specialists to rural geographic regions.
Technology Acceptance Model and Theoretical Framework
The theoretical concept of this study, as suggested by Davis, the Technology Acceptance Model (TAM), is that perceived usefulness and perceived ease of use are the main factors that determine technology adoption intention [21].
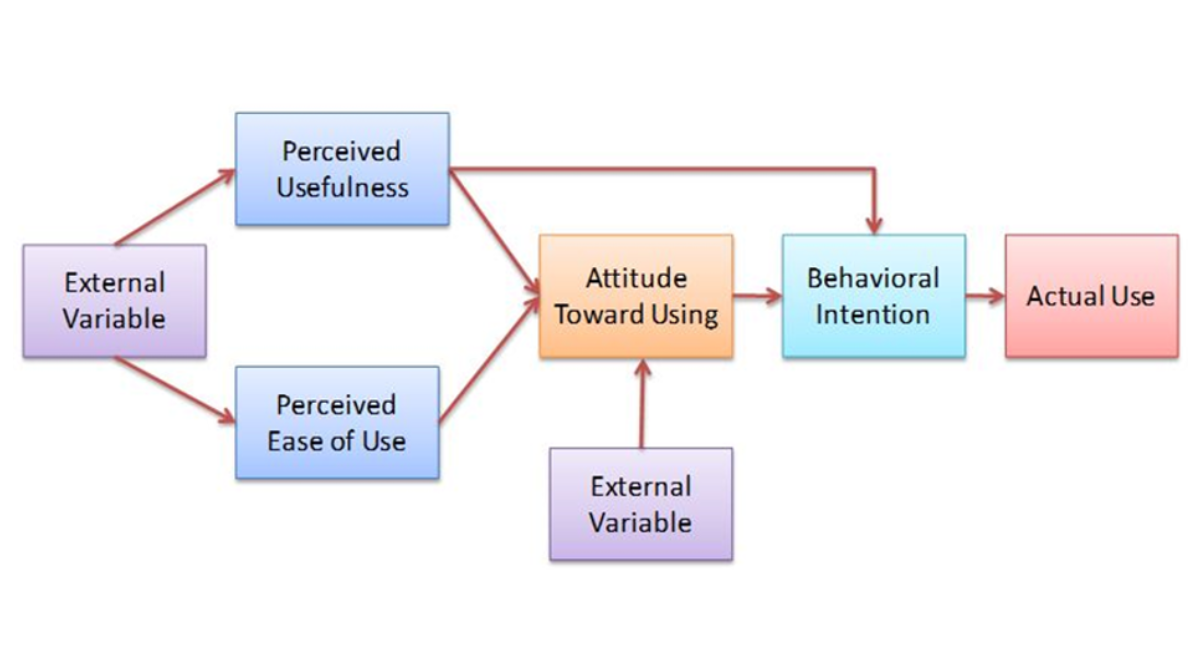
Figure 1: The Technology Acceptance Model (TAM)
Some of the follow-ups that include trust, security, and infrastructure preparedness are especially applicable in the LMICs, which still have a nascent institutional trust in digital systems [22]. According to Mbunge from Kenya, Devi from India and Raza from Pakistan, the explanatory utility of TAM is maintained by research in additional emerging economy conditions [2,6,23]. The study also identifies context-specific moderators (e.g. digital literacy, cost barriers, and regulatory frameworks). This paper builds upon the TAM, introducing the quality of infrastructure and data governance as the two new constructs of the Bangladeshi digital health ecosystem.
MATERIALS AND METHODS
Research Design and Approach
The research design that is taken in this study is a positivist, quantitative research design based on primary data collection. The methodology of the study was a cross-sectional survey that aimed at determining the impact of AI, Big Data, and IoT technologies on the digital quality of healthcare in Bangladesh. The study sample included healthcare providers, hospital leaders, patients who were using digital health services and health-technology innovators in four large divisions: Dhaka, Chittagong, Rajshahi, and Sylhet.
Sampling and Data Collection
The sampling and data collection will involve the inclusion of 385 participants. A sample of 385 was calculated by using the formula provided by Yamane of 95% confidence level and a 5% margin of error, where the population is approximated to be 20,000 digital health stakeholders [24]. The stratified random method of sampling was used in order to have proportional representation of the stakeholder groups. The questionnaires will be self-administered in a structured and five-point Likert scale with a pilot test conducted on 30 respondents to achieve a Cronbach's Alpha of 0.847, which indicates high internal consistency. The questionnaire consisted of four parts of constructs, namely: AI application in diagnostics (8 items), Big Data utilisation in health management (7 items), IoT integration in patient monitoring (8 items), and digital health service quality (10 items), and demographic variables.
Data Analysis
The 385 coded and analysed usable questionnaires were analysed with the IBM SPSS Statistics Version 26. The analysis was carried out in four steps namely: (1) descriptive statistics to profile the demographics and characterise the variables; (2) reliability analysis (Cronbachs Alpha); (3) Pearson correlation as a measure of the relationship between the constructs; and (4) Multiple linear regression to ascertain the relative predictive power of AI, Big Data, and IoT on digital health service quality, with multicolline.
RESULTS AND FINDINGS
Demographic Profile of Respondents
Table 1 shows the social demographic values of the 385 respondents. The study sample was mainly male (58.4 per cent), although 41.6 per cent of the sample consisted of females. Most of them (46.2) were between the ages of 31 and 45 years. The highest stakeholder group (34.3% was comprised of the medical personnel, patients who used digital health services (29.6%), hospital administrators (22.1%), and technology developers (14.0%). The proportion of persons who had a bachelor's degree or above was very high (61.0), and this demonstrated that the sample had a relatively high level of education. The respondents were the highest in Dhaka Division (42.3%), which is the same variation as the concentration of healthcare institutions.
|
Variable |
Category |
Frequency |
Percentage (%) |
|
Gender |
Male |
225 |
58.4 |
|
Female |
160 |
41.6 |
|
|
Age Group |
18–30 years |
98 |
25.5 |
|
31–45 years |
178 |
46.2 |
|
|
46–60 years |
89 |
23.1 |
|
|
Above 60 years |
20 |
5.2 |
|
|
Stakeholder Type |
Healthcare Professional |
132 |
34.3 |
|
Patient |
114 |
29.6 |
|
|
Hospital Administrator |
85 |
22.1 |
|
|
Technology Developer |
54 |
14 |
|
|
Education Level |
Secondary / Higher Secondary |
150 |
39 |
|
Bachelor's Degree |
155 |
40.3 |
|
|
Postgraduate & Above |
80 |
20.7 |
|
|
Division |
Dhaka |
163 |
42.3 |
|
Chittagong |
89 |
23.1 |
|
|
Rajshahi |
74 |
19.2 |
|
|
Sylhet |
59 |
15.4 |
Table 1: Demographic Profile of Respondents (N = 385)
Reliability and Descriptive Statistics
Reliability studies ensured the internal consistency of all constructs, where Cronbach's Alpha coefficient of 0.831 to 0.876 was all well above the acceptable level of 0.70 [25]. Table 2 shows the descriptive statistics and reliability coefficients of each construct. The mean scores of all four constructs were above the scale mid (3.00), which is why in general the quality of the perceptions of AI, Big Data, IoT, and the quality of digital health services are favourable among the respondents. The highest mean score (M = 3.91, SD = 0.72) was registered in the AI Application in Diagnostics, which implies that the respondents are highly aware of the diagnostic potential of AI. Digital Health Service Quality registered the average of 3.84 (SD = 0.68), which indicated moderate-high satisfaction with the existing digital health services.
|
Construct |
Items |
Mean |
Std. Dev. |
Cronbach's α |
|
AI Application in Diagnostics |
8 |
3.91 |
0.72 |
0.868 |
|
Big Data Utilisation in Health Management |
7 |
3.74 |
0.81 |
0.843 |
|
IoT Integration in Patient Monitoring |
8 |
3.82 |
0.76 |
0.876 |
|
Digital Health Service Quality |
10 |
3.84 |
0.68 |
0.831 |
Table 2: Descriptive Statistics and Reliability Analysis
Pearson Correlation Analysis
Analysis of Pearson correlation (Table 3) showed that there was a statistically significant positive correlation between all the constructs of the study (p < 0.01). AI Application and Digital Health Service Quality showed a positive correlation with its value of 0.681, which is significantly less than 0.05 (r = 0.681, p < 0.001), meaning that improved quality of service provision in terms of AI adoption is highly interconnected with the improvement of the latter. There was the highest correlation of IoT Integration with the dependent variable (r = 0.712, p < 0.001), which shows the critical role of real-time remote monitoring in the improvement of service delivery. Significant positive correlation (r = 0.643, p < 0.001) was also observed in the Big Data Utilisation. The inter-predictor correlations were between 0.514 and 0.598, and this value is below the value of concern (r = 0.80), hence it is possible to say that there is no multicollinearity between independent variables.
|
Variable |
1. AI |
2. Big Data |
3. IoT |
4. DHSQ |
|
1. AI Application |
1 |
|||
|
2. Big Data Utilisation |
0.568** |
1.000 |
||
|
3. IoT Integration |
0.598** |
0.514** |
1000 |
|
|
4. Digital Health Service Quality |
0.681** |
0.643** |
0.712** |
1000 |
Table 3: Pearson Correlation Matrix
Note: **Correlation is significant at the 0.01 level (2-tailed). DHSQ = Digital Health Service Quality.
Multiple Regression Analysis
The Digital Health Service Quality (DHSQ) was taken as a dependent variable, and AI Application, Big Data Utilisation, and IoT Integration as independent variables in the multiple linear regression analysis. The overall model was statistically significant (F(3, 381) = 352.41, p < 0.001), explaining 73.4% of the variance in DHSQ (R² = 0.734, Adjusted R² = 0.731). The three technological constructs can explain the findings. The standardised regression coefficients are shown in Table 4.
|
Predictor |
B (Unstd.) |
Std. Error |
β (Std.) |
t-value |
Sig. |
VIF |
|
(Constant) |
0.421 |
0.118 |
– |
3.568 |
0.000 |
– |
|
AI Application |
0.362 |
0.049 |
0.381 |
7.388 |
0.000 |
1.641 |
|
Big Data Utilisation |
0.271 |
0.051 |
0.297 |
5.314 |
0.000 |
1.512 |
|
IoT Integration |
0.398 |
0.047 |
0.412 |
8.468 |
0.000 |
1.719 |
Table 4: Multiple Regression Analysis Results (Dependent Variable: Digital Health Service Quality)
Note: R = 0.857; R² = 0.734; Adjusted R² = 0.731; F(3, 381) = 352.41; p < 0.001. All VIF values < 2.0, confirming no multicollinearity.
The most predictive of the digital health service quality were found to be IoT Integration (0.412, p < 0.001), AI Application (0.381, p < 0.001) and Big Data Utilisation (0.297, p < 0.001). Predictors of all the predictors were statistically significant (p < 0.001). The values of the Variance Inflation Factor (VIF) of all predictors were less than 2.0, which is well within acceptable limits (VIF < 10), which proved that there was no multicollinearity.
Barriers to AI, Big Data, and IoT Adoption in Digital Healthcare
In addition to the regression model, the respondents were required to individually rate the severity of the identified barriers to the digital health technology adoption on a five-point Likert scale (1 = Not a barrier; 5 = Critical barrier). The mean barrier ratings sorted by their severity are shown in Table 5.
|
Barrier |
Mean |
Std. Dev. |
Rank |
|
Inadequate digital infrastructure (internet, power) |
4.38 |
0.61 |
1 |
|
Data privacy and cybersecurity concerns |
4.21 |
0.69 |
2 |
|
Limited digital health literacy among patients |
4.09 |
0.74 |
3 |
|
Insufficient government regulatory frameworks |
3.96 |
0.78 |
4 |
|
High implementation and maintenance costs |
3.88 |
0.81 |
5 |
|
Resistance from healthcare professionals |
3.64 |
0.87 |
6 |
|
Interoperability issues across health systems |
3.52 |
0.91 |
7 |
|
Lack of qualified health-IT professionals |
3.47 |
0.94 |
8 |
Table 5: Barriers to Digital Health Technology Adoption (Ranked by Mean Score)
The most important barrier was infrastructure deficiency, including unreliable internet connection and unreliable electricity supply (M = 4.38, SD = 0.61), especially when it comes to the deployment of IoT remote monitoring in rural areas. In the second place (M = 4.21) were data privacy and cybersecurity concerns that show an increased level of understanding of the vulnerabilities of digital health data. The third most relevant barrier has been found to be the limited patient digital literacy (M = 4.09), which impedes the proper patient interaction with AI-powered and IoT-based services. The comparatively lower score of professional resistance (M = 3.64) indicates the growing acceptance of digital tools by the Bangladeshi healthcare professionals, which is in line with the post-pandemic attitudinal changes that have been recorded in the region.
Respondent Perceptions of Technology Benefit Domains
The respondents were also requested to answer the question about the area of healthcare where they believed that AI, Big Data, and IoT would be the most useful. The greatest percentage (32.7%) was assigned to diagnostic accuracy, next comes chronic disease management (24.2%), disease surveillance and outbreak detection (18.4%), administrative efficiency (14.0%), and drug supply chain management (10.7%). These results are in line with those of a regression that focused on the importance of the IoT in unremitting monitoring of patients with chronic conditions, and AI's role as a focal point in diagnostic-based applications.
DISCUSSION
The results of the research provide strong empirical evidence of the transformational potential of AI, Big Data, and IoT in a digital healthcare environment in Bangladesh. The explanatory power of the regression model (R 2 = 0.734 ) is significantly higher than that of similar studies in analogous LMIC settings, as Mbunge found that R 2 of 0.61 indicated the deployment of digital health in South Africa, and Raza found R 2 of 0.67 in the Pakistani settings [2,6].
The fact that IoT Integration is the most significant individual predictor (= 0.412) is theoretically right because the literature on the subject of IoMT is steadily growing, and practically valid since the rate of mobile penetration in Bangladesh is high (96%), which is an initial layer of connectivity that enables the implementation [7,19]. The capacity to offer constant physiological care to hypertensive and diabetic people in rural upazilas without the need to visit the hospital, physically, is especially high-impact of the service in Bangladesh due to the prevalence of chronic diseases in the country [3].
The high predictive coefficient (0.381) of the AI Application supports the international findings on the diagnostic efficacy of AI Rajpurkar and is especially relevant in the given case, where the ratio of specialists to patients in rural regions reaches 1:50,000. Triage and diagnostic decision support systems with AI applications implemented at Upazaka Health Complexes can significantly reduce this disparity of access [8]. The significant yet relatively small coefficient of the Big Data Utilisation (=0.297) is probably the indicator of the infantile stage of health data infrastructure development in Bangladesh, when the national EHR adoption has not been fully developed yet, and data pools required to build quality analytics are still disconnected.
The barrier profile that is largely characterised by the lack of infrastructure and data privacy issues aligns with the rest of the LMIC digital health literature and creates an understanding that there is no single solution to the barrier issue, which can solely be technology implementation [18,23]. By investing in power infrastructure, the expansion of broadband over 5G, sustainable digital transformation of health is possible. The extension of the TAM-based framework of the study, including the infrastructure quality and data governance as the context-dependent constructs, therefore, makes a valuable contribution to the theoretical growth in the context of LMIC digital health research.
RECOMMENDATIONS
The policy and practice recommendations, based on the findings of the empirical results, are promoted to the Government of Bangladesh, healthcare institutions and technology stakeholders:
Ministry of Health and Family Welfare (MOHFW) needs to come up with a National AI in Healthcare Strategy, which would provide a clear regulatory avenue in approving AI diagnostic tools, certifying medical IoT devices, and setting up standards of governance of big data regarding health information [4]. A complete Digital Health Data Protection Act in line with the international best practices is well-timed to be enacted to mitigate the cybersecurity issues that are ranked second as a barrier.
As part of Smart Bangladesh Vision 2041, the Government should focus on last-mile connectivity infrastructure that will be expanded to cover rural Upazila Health Complexes, which are important deployment locations of IoT patient monitoring. The state-company collaboration with technical companies, an example of which can be seen in Bangladesh in the case of mobile financial services, should be used to fund the introduction of health-IoT infrastructures. Clinical and administrative staff and structured digital health literacy programmes should be invested in by healthcare institutions for patients. The Telemedicine systems with both AI-based symptom checkers and IoT biosensors connections should be expanded via the already existing Community Clinic network in Bangladesh. Lastly, academic-industry consortia are needed to create a national health-IT workforce, which can create and support context-relevant digital health solutions and decrease their reliance on imported technology in the long term.
CONCLUSION
The present research is a solid piece of quantitative data demonstrating that the combined use of AI, Big Data, and IoT technologies can be considered a potent tool that will allow improving the quality of digital healthcare in Bangladesh. Taken together, all of these technologies contribute to 73.4 per cent of the digital health service quality variance, with the use of IoT, AI applications, and big data turning out to be statistically significant and practically relevant predictors. These results place Bangladesh and, therefore, other similar emerging economies such as these in a position where technology-based healthcare leapfrogging is not only possible but also empirically viable.
The Bangladesh Digital Health Framework (BDHF), which is a part of the study but based on an extended TAM and empirically proven by primary data (385 stakeholders in four divisions), provides an evidence-based model that can be replicated to make substantial changes in the digital health policy formulation. It will be necessary to bring together the twin needs of infrastructure growth and data management to transform the inherent potential in technology into fair health outcomes for Bangladesh, which has 170 million people. Future studies need to investigate the longitudinal health outcomes after technology implementation, the cross-national comparative studies in South Asia, and the actual effect of AI diagnostic devices on the accuracy of decisions of clinicians in low-resource Bangladeshi environments.
REFERENCES
- Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nature medicine. 2019 (1):44-56. [Crossref] [Google Scholar] [PubMed]
- Raza K, Toor S, Munawar HS & Ahmad F. (2022). Internet of Things-based smart health framework for disease diagnosis. IEEE Access, 10, 34900–34916.
- World Health Organisation (WHO). (2023). Bangladesh: WHO statistical profile. WHO Regional Office for South-East Asia.
- Ministry of Health and Family Welfare (MoHFW). (2022). Health, population and nutrition sector program (HPNSP) 2017–2022 implementation report. Government of Bangladesh.
- Bangladesh Telecommunication Regulatory Commission (BTRC). (2023). Annual report on mobile and internet penetration in Bangladesh. BTRC Publications.
- Mbunge E, Akinnuwesi B, Fashoto SG, Metfula AS, Mashwama P. A critical review of emerging technologies for tackling COVID‐19 pandemic. Human behavior and emerging technologies. 2021 (1):25-39. [Crossref] [Google Scholar] [PubMed]
- Javaid M, Haleem A, Singh RP, Suman R, Rab S. Significance of machine learning in healthcare: Features, pillars and applications. International Journal of Intelligent Networks. 2022;3:58-73. [Crossref] [Google Scholar]
- Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nature medicine. 2022;28(1):31-8. [Crossref] [Google Scholar] [PubMed]
- Shen D, Wu G, Suk HI. Deep learning in medical image analysis. Annual review of biomedical engineering. 2017;19:221-48. [Crossref] [Google Scholar] [PubMed]
- Esteva A, Kuprel B, Novoa RA, Ko J, Swetter SM, et al. Dermatologist-level classification of skin cancer with deep neural networks. nature. 2017;542(7639):115-8. [Crossref] [Google Scholar] [PubMed]
- Jiang F, Jiang Y, Zhi H, Dong Y, Li H, et al. (2017). Artificial intelligence in healthcare: Past, present and future. Stroke Vasc Neurol, 2(4), 230–243. [Crossref] [PubMed]
- Obermeyer Z, Emanuel EJ. Predicting the future—big data, machine learning, and clinical medicine. The New England journal of medicine. 2016;375(13):1216. [Crossref] [Google Scholar] [PubMed]
- Raghupathi W, Raghupathi V. Big data analytics in healthcare: promise and potential. Health information science and systems. 2014;2(1):3. [Crossref] [Google Scholar] [PubMed]
- Thew J. (2016). Big data means big potential, challenges for nurse execs. HealthLeaders Media.
- Shameer K, Johnson KW, Glicksberg BS, Dudley JT, Sengupta PP. Machine learning in cardiovascular medicine: are we there yet?. Heart. 2018;104(14):1156-64. [Crossref] [Google Scholar]
- Chen H, Chiang RH, Storey VC. Business intelligence and analytics: From big data to big impact. MIS quarterly. 2012;36(4):1165-88. [Crossref] [Google Scholar]
- Directorate General of Health Services (DGHS). (2022). Health Bulletin 2022. Ministry of Health and Family Welfare, Bangladesh.
- Ahad MA, Paiva S, Tripathi G, Feroz N. Enabling technologies and sustainable smart cities. Sustainable cities and society. 2020;61:102301. [Crossref] [Google Scholar]
- Islam SR, Kwak D, Kabir MH, Hossain M, Kwak KS. The internet of things for health care: a comprehensive survey. IEEE access. 2015;3:678-708. [Crossref] [Google Scholar]
- Bhatt C, Dey N, Ashour AS, editors. Internet of things and big data technologies for next generation healthcare. [Crossref] [Google Scholar]
- Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS quarterly. 1989;13(3):319-40. [Crossref] [Google Scholar]
- Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of information technology: Toward a unified view1. MIS quarterly. 2003;27(3):425-78. [Crossref] [Google Scholar]
- Devi BR, Syed-Abdul S, Kumar A, Iqbal U, Nguyen PA, et al. mHealth: An updated systematic review with a focus on HIV/AIDS and tuberculosis long term management using mobile phones. Comput Methods Programs Biomed. 2015;122(2):257-65. [Crossref] [Google Scholar] [PubMed]
- Yamane T. Statistics: An introductory analysis. [Google Scholar]
- Nunnally JC. Psychometric Theory 2nd ed. Mcgraw hill book company. [Crossref] [Google Scholar]
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 25-35 Days |
Peer Review Feedback |
| 45-60 Days | Total article processing time |
Why Publish with us?
Ethics & Policies
Editorial & Management
Useful Links
Journal Highlights
Open Access Journals
Membership
Journal Flyer