ABSTRACT
Background
The assessment of operability in children with non-restrictive left to right shunt lesions presenting with severe pulmonary arterial hypertension (PAH) typically relies on pulmonary vascular resistance index (PVRI). However, pulmonary artery compliance (Cp) remains underutilized.
Objectives
This study aimed to describe Cp values in this population, evaluate their relationship with conventional hemodynamic parameters, and establish cut-off values for Cp in basal and oxygen studies.
Methods
This was a single-center retrospective analysis done in children with non-restrictive left to right shunt lesions with severe PAH, who underwent cardiac catheterization from March 2018 to August 2025. Patients with basal PVRI more than 6 wuxm2 were included in the study. The cohort was divided into two groups, group A - patients who were operated and group B – patients who were managed medically. The Cp was calculated retrospectively in both the groups.
Results
A total of 63 patients were included in this analysis. Group A had significantly higher basal Cp values compared to Group B (mean basal Cp: 1.12 ±0.47 vs. 0.66 ±0.16 ml/mmHg/m², p < 0.01). Cp showed strong positive correlation with indexed pulmonary blood flow and strong negative correlation with PVRI.
Conclusion
This study provides normative Cp values and thresholds in children with severe PAH due to non-restrictive VSD or PDA. Cp correlated strongly with conventional hemodynamic indices, and the identified cut-off values may serve as useful reference points. However, prospective outcome-based studies are required to clarify its role in surgical decision-making.
Keywords: Pulmonary Artery Hypertension; Pulmonary Artery Compliance; Ventricular Septal Defect; Patent Ductus Arteriosus; Oximetry Analysis; Pulmonary Vascular Resistance Index
INTRODUCTION
Patients with a non-restrictive ventricular septal defect (VSD) and patent ductus arteriosus (PDA) are subjected to surgical closure early in life, around 4 to 6 months of age, on the basis of clinical history, physical examination, chest X-ray, and echocardiographic analysis. This ideal age of surgery is not the case in developing countries, and encountering such patients beyond the ideal age for surgery is not uncommon. Thus, for patients who present beyond 2 years of age, invasive hemodynamic analysis is recommended to assess the pulmonary vasculature [1]. Among the hemodynamic parameters, pulmonary vascular resistance index (PVRI) is given the most weightage [2,3].
But the pulmonary vasculature has 3 components, i.e.; the PVRI, pulmonary artery compliance (Cp) and impedance. The PVRI represents the static right ventricular (RV) afterload, and impedance and compliance are the dynamic components of the afterload [4]. The importance of Cp has been overlooked in non-restricted left to right shunt lesions with severe PAH. There have been only a few studies which assessed Cp in congenital heart disease [5,6]. It has recently been shown that lower Cp is strongly associated with worse survival in adult patients with PAH [7]. However, despite its potential importance to RV performance and clinical outcomes, Cp is not routinely measured in children with PAH. This study aimed to describe Cp values in this population, evaluate their relationship with conventional hemodynamic parameters, and establish cut-off values for Cp in basal and oxygen studies.
METHODS
This was a retrospective analysis conducted at a tertiary care pediatric cardiac center. The cardiac catheterization data of patients with a non-restrictive VSD and PDA who were admitted between April 2018 and August 2025 for oximetry analysis were reviewed. Patients with a basal PVRI > 6 Wood units x m² were included in the final analysis. Those with branch pulmonary artery abnormalities or associated lung disease were excluded. Ethics committee approval was not taken, and informed consent was taken from the parents before the procedure.
Cardiac catheterization procedure: Cardiac catheterization was performed under conscious sedation. After securing femoral arterial line, an initial arterial blood gas was done to rule out metabolic acidosis or hypercarbia. Routine basal hemodynamic parameters were calculated. Oxygen consumption was estimated using the Lafarge and Miettinen chart [8]. For patients where pulmonary capillary wedge pressure was not recorded, left ventricular end-diastolic pressure was used to calculate PVRI. The pulmonary arterial pressures were obtained by averaging several consecutive beats. In PDA cases, the pulmonary artery saturations were obtained from both branch pulmonary arteries, and the values were averaged.
Vasoreactivity testing was performed using 100% oxygen (via a non-rebreathing face mask) for 10 minutes, and the same hemodynamic parameters were reanalyzed. The decision regarding operability was based on the complete clinical picture, which included age, history, clinical examination, chest X-ray, electrocardiogram, and hemodynamic data. A combined clinical decision involving the surgical team was made to determine operability. The main criteria for going ahead with surgery were age younger than 2 years, echo features of LA/LV dilatation, basal saturation more than 92, clinical features of increased pulmonary blood flow and failure to thrive. Based on the treatment plan, patients were categorized into two groups:
Group A: Operated and Group B: Medical management
Then Cp was calculated retrospectively for both basal data and on oxygen for both the groups. Cp was determined using the pulse pressure method as shown in the formula below [9-12]
Cp = Pulmonary blood flow indexed to body surface area (Qp) / (Heart rate × Pulmonary artery pulse pressure)
Statistical Analysis
Data was represented as mean ± standard deviation (SD), median or frequency (percentage). The data was tested for normality by applying the Kolmogorov-Smirnov test. The hemodynamic parameters were compared between the Group A and B using unpaired t-test for normally distributed data and the Mann-Whitney U test for non-normally distributed parameters. Similarly, the hemodynamic data was compared between baseline and on oxygen study using the paired t-test. Correlation analysis between Cp and other hemodynamic parameters was conducted using Pearson's correlation coefficient to assess the strength and direction of their linear relationships. The Receiver operating characteristic (ROC) curves were generated to identify the cut-offs for Cp (basal and on oxygen study) and its percentage increase after oxygen study. P-value of < 0.05 was taken as significant.
RESULTS
Baseline Characteristics
A total of 162 patients of non-restricted VSD and PDA underwent oximetry in our center. Out of these, 63 patients had basal PVRI > 6 wood units x m2 and were included in the study group. The mean age was 6.99 ± 3.82 years (median = 6 years) and mean weight was 16.9 ± 7.4 kg (median = 16.4 kg). There were 45 patients of VSD and 18 patients of PDA.
Hemodynamic Parameters for the Whole Group
The basal Cp of the whole study group was 0.94 ± 0.45 (0.86) ml/mmHg/m² on basal study and Cp on oxygen was 1.8 ± 0.87 (1.7) ml/mmHg/m², which was a statistically significant increase as shown in table 1. The percentage increase in Cp for the whole group after oxygen study was 98.3%. There was a statistically significant reduction in systolic, diastolic and mean pulmonary artery (PA) pressures on oxygen study. Also, there was a significant increase in Qp, Qp:Qs ratio and reduction in PVRI and Rp:Rs ratio.
|
Parameters |
Basal |
On oxygen |
P value |
|
SBP (mmHg) |
105.5 ± 19.4 (105) |
98.8 ± 20.1 (100) |
< 0.01 |
|
DBP (mmHg) |
51.1 ± 15.2 (50) |
44.7 ± 16.1 (45) |
< 0.01 |
|
MBP (mmHg) |
76.3 ± 13.8 (79) |
69.5 ± 16.4 (70) |
< 0.01 |
|
PP (mmHg) |
54.1 ± 12.4 (54) |
54.1 ± 12.1 (55) |
0.96 |
|
Heart rate |
114.1 ± 17.1 (115) |
108.2 ± 17.8 (106) |
< 0.01 |
|
Qp |
5.51 ± 2.1 (5.1) |
10 ± 3.7 (10) |
< 0.01 |
|
Qs |
4.28 ± 0.95 (4.1) |
3.7 ± 1.4 (3.5) |
0.01 |
|
Qp:Qs ratio |
1.35 ± 0.58 (1.2) |
2.9 ± 1.4 (2.6) |
< 0.01 |
|
PVRI (wuxm2) |
14.1 ± 6.2 (12.5) |
7.3 ± 3.8 (5.8) |
< 0.01 |
|
SVRI (wuxm2) |
19.4 ± 4.9 (18.7) |
22.8 ± 7.2 (22.3) |
0.01 |
|
Rp:Rs ratio |
0.77 ± 0.42 (0.66) |
0.34 ± 0.27 (0.3) |
< 0.01 |
|
Cp (ml/mmHg/m²) |
0.94 ± 0.45 (0.86) |
1.8 ± 0.87 (1.7) |
< 0.01 |
Table 1: Hemodynamic Parameters for the Whole Group
Comparison between Groups
There were 33 patients in Group A (VSD = 26 and PDA = 7) and 30 patients in Group B (VSD = 19 and PDA = 11). The mean age in Group A was 5.9 ± 3.0 (median = 5) years, which was significantly lower than Group B, which was 8.7 ± 3.49 (median = 8.25) years, with a p value of < 0.01. The mean basal Cp was 1.12 ± 0.47 (median = 1.05) ml/mmHg/m² in Group A, and it was significantly lower in Group B, i.e. 0.66 ± 0.16 (median = 0.64) ml/mmHg/m². Similarly, the mean basal PVRI in Group A was lower than that of Group B, which was statistically significant.
Comparison of Basal Vs on Oxygen Study in Group A
There was a statistically significant reduction in PA pressures, PVRI, Rp:Rs ratio and increase in Qp:Qs ratio and Cp during the oxygen study with respect to basal study in Group A. The median percentage increase in Cp was 110.48% as shown in figure 1. All of the patients had a reduction in PVRI of > 20 % with a final value to < 6 wood units x m2 and Rp:Rs ratio less than 0.3.
Comparison of Basal Vs on Oxygen Study in Group B
In Group B, there was statistically significant reduction in systolic PA pressure, but the diastolic pressure did not show a significant reduction on oxygen study. There was a statistically significant increase in Qp:Qs ratio and Cp and reduction in PVRI and Rp:Rs ratio on oxygen when compared to basal study. But in this group the PVRI didn’t fall to less than 6 wood units / m2 on oxygen study. The median percentage increase in Cp was 75.05% as shown in figure 1.
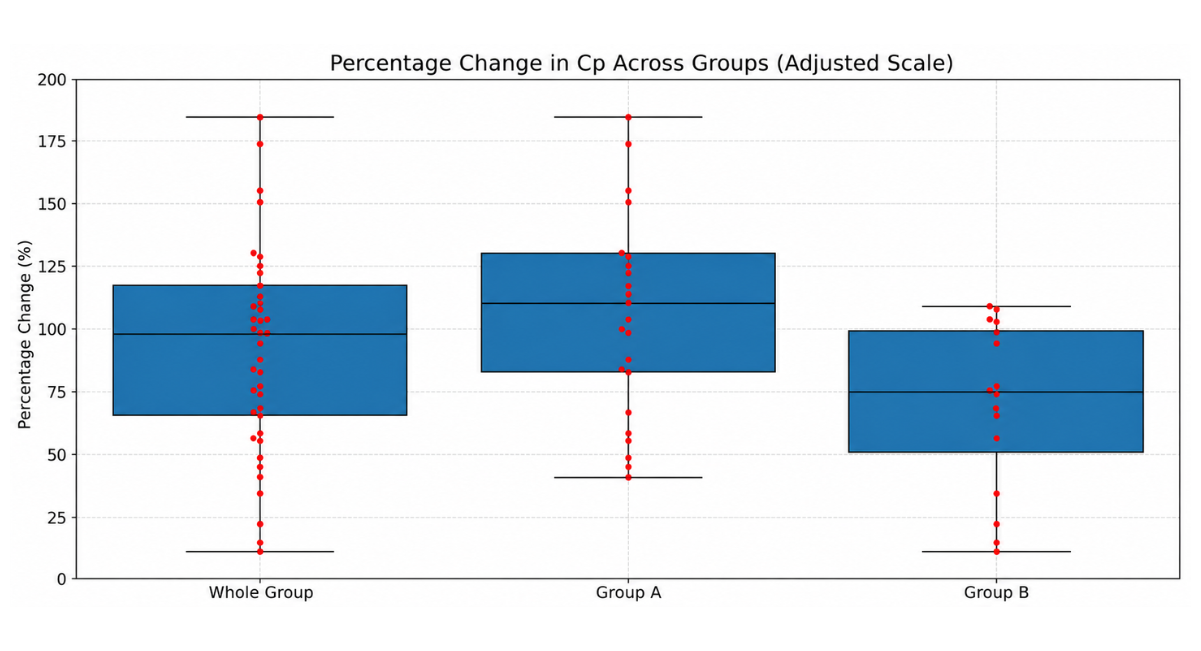
Figure 1: Figure Shows Box Plot of Percentage Change in Cp
Correlation Of Cp with Other Hemodynamic and Demographic Parameters
There was a strong positive correlation between Cp and Qp (r = 0.87, p < 0.001), Qp:Qs ratio (r = 0.82, p < 0.001) and a strong negative correlation with PVRI (r = -0.69, p < 0.001) and Rp:Rs ratio (r = -0.65, p < 0.001). Among the pulmonary artery pressures, there was a moderate negative correlation of Cp with PP (r = -0.49, p = 0.001), but only weak negative correlations with SBP, DBP and MBP (r = -0.33, p = 0.037; r = -0.15, p = 0.337 and r = -0.03, p = 0.872 respectively). Also, there was negligible correlation of Cp with heart rate (r = 0.01, p = 0.951).
Demographic factors such as age, height, weight and type of lesion exhibited weak correlations with Cp (|r| < 0.16) and were not statistically significant (p > 0.05).
Operability Assessment Based on Cp
The assessment of operability using Cp was done by analysis of ROC curves for Cp at baseline, on oxygen study and percentage increase of Cp as shown in figure 2.
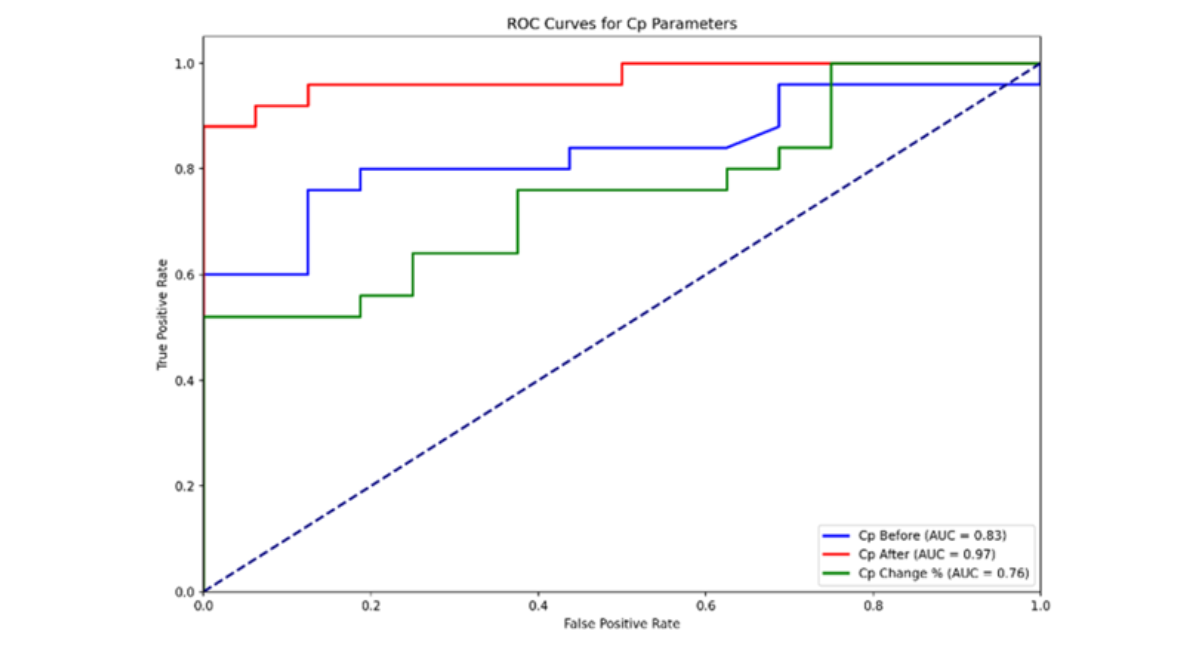
Note: Cp Before = Basal Cp, Cp After = Cp on Oxygen Study, Cp Change % = Percentage Change in Cp from Basal to Oxygen Study
Figure 2: Figure Showing ROC Curves for Basal Cp, Cp After Oxygen Study and Percentage Change in Cp
The analysis identified an optimal threshold for basal Cp at 0.86 ml/mmHg/m² for operability, with a sensitivity of 0.76, specificity of 0.88, and an area under the curve (AUC) of 0.83, demonstrating good discriminatory capacity. Following the oxygen study, the optimal threshold for Cp increased significantly to 1.67 ml/mmHg/m², with improved sensitivity of 0.88, perfect specificity of 1.00, and an AUC of 0.97, indicating excellent predictive accuracy. Additionally, the percentage change in Cp revealed an optimal threshold of 110.48%, with a sensitivity of 0.52, specificity of 1.00, and an AUC of 0.76, reflecting its utility as a specific but moderately sensitive marker for operability.
DISCUSSION
Currently, operability in children presenting beyond the ideal age for surgery is determined by hemodynamic parameters, of which PVRI is given the most weightage. Cp, which is the other face of the coin of pulmonary vascular bed, is usually not included in the analysis traditionally, and there are no cut-off values for operability during both basal and oxygen studies. We aimed to analyze the Cp in this cohort, to find its correlation with other hemodynamic parameters and to derive a cut-off value of Cp for operability.
In this study, the mean Cp for the whole study group was 0.94 ±0.45 (median = 0.86) ml/mmHg per m². As all of our patients had severe PAH (with PVRI > 6 WU×m²), it was expected that the Cp would be lower compared to those without PAH. Similar findings were reported in a study by Chaubey, where the mean Cp for the overall study group was 2.88 ml/mmHg per m². In the inoperable group, the mean Cp was 0.61 ml/mmHg/m², and in borderline patients, it was 0.87 ±0.3 ml/mmHg/m². Our patient cohort was similar to the borderline group and inoperable group of patients in this study.
Group-wise analysis showed that Group A (operated) patients were significantly younger, had higher Cp (both basal and on oxygen), and lower PVRI compared to Group B (not operated) patients. Additionally, the percentage increase in Cp in Group A was greater compared to Group B (110.48% vs. 75.05%). This indicated that the effect of oxygen in increasing pulmonary blood flow was more pronounced in Group A patients, suggesting a more reactive pulmonary vascular bed in these patients.
Correlation of Cp with other hemodynamic parameters was also analyzed. A strong positive correlation was seen with Qp and Qp:Qs ratio, and a strong negative correlation was observed with PVRI and Rp:Rs ratio. Similar findings were reported in a study by Muneuchi, which showed an inverse parabolic relationship between Cp and PVRI and a positive relationship with Qp:Qs ratio [13]. The relationship between Cp and various PA pressures was negative but not strong enough to be significant, which aligns with findings from the study by Chaubey [6].
Operability was assessed using ROC curve analysis for Cp and its percentage increase, as shown in Figure 2. In this study, a basal Cp cut-off of 0.86 ml/mmHg/m² was identified for predicting operability, while oxygen-derived Cp (>1.67 ml/mmHg/m²) demonstrated superior discriminatory performance. These values are lower than those reported in previous pediatric studies evaluating pulmonary vascular disease and operability.
Muneuchi evaluated pulmonary arterial compliance in infants with congenital heart disease and reported a Cp threshold of <1.22 ml/mmHg/m² for predicting significant pulmonary vascular disease, with high sensitivity (93%) but modest specificity (64%) [14]. Similarly, Chaubey et al. studied a broader and more heterogeneous cohort ranging from infants to adults with various left-to-right shunt lesions and reported a higher Cp cut-off of <1.18 ml/mmHg/m² for inoperability, with excellent diagnostic accuracy (AUC 0.99) [6]. Compared with both studies, our lower basal Cp cut-off (0.86 ml/mmHg/m²) likely reflects the inclusion of a more advanced disease spectrum, as all patients in our cohort had severe pulmonary arterial hypertension with PVRI >6 WU×m² and were, therefore, already preselected for significant pulmonary vascular remodeling.
In addition, differences in lesion distribution and age may significantly influence Cp thresholds. The study by Muneuchi primarily included very young infants (median age ~4 months), in whom pulmonary vascular compliance is physiologically higher and more dynamic, potentially resulting in higher absolute Cp cut-offs for disease discrimination [13,14]. In contrast, the Chaubey et al. cohort included a wide age range (2 months to 70 years) with a predominance of atrial septal defect physiology, where chronic volume loading rather than advanced obstructive pulmonary vascular disease may dominate vascular mechanics. This heterogeneity likely contributed to their relatively higher Cp threshold compared with the present study, which predominantly reflects older children with established severe pulmonary vascular disease.
Furthermore, none of the previously published studies have evaluated oxygen-induced changes in Cp or percentage increase in Cp as a marker of operability. The present study is therefore the first to demonstrate that oxygen reactivity of Cp provides incremental discriminatory value, with a >110% increase showing high specificity for operability. This suggests that dynamic Cp assessment may better capture pulmonary vascular recruitability compared to static single-point measurements alone, particularly in borderline patients where PVRI alone may be inconclusive.
Taken together, these findings suggest that Cp thresholds are not fixed physiological constants but are highly dependent on age, lesion type, disease severity, and study design. Therefore, Cp cut-off values should be interpreted within the clinical and hemodynamic context rather than applied universally across populations.
From a clinical perspective, Cp should be viewed as a complementary rather than a replacement parameter for PVRI. While PVRI reflects the resistive component of the pulmonary circulation, Cp provides additional information regarding the pulsatile component of right ventricular afterload, thereby offering a more comprehensive assessment of pulmonary vascular physiology. An important practical advantage of Cp is that it can be calculated from routinely obtained catheterization data without requiring additional equipment, procedural time, or cost. In patients with borderline operability, particularly those with intermediate PVRI values, Cp may provide supportive physiological information. Furthermore, the marked increase in Cp during oxygen administration observed in operable patients suggests that dynamic changes in compliance may reflect pulmonary vascular recruitability, offering insights beyond static resistance measurements alone [15]. However, prospective studies are needed to determine whether incorporating Cp into routine operability assessment improves clinical decision-making and long-term outcomes.
LIMITATIONS
This study’s retrospective design and single-center data may limit the generalizability of the findings. Furthermore, we assumed that the decision to operate or not was correct, and based on this assumption we calculated the cut-off of Cp for operability, which is a major limitation.
CONCLUSION
In conclusion, this study identified Cp thresholds that aligned with previous operability decisions in patients with VSDs, PDAs, and severe pulmonary hypertension, based on traditional criteria. While Cp demonstrates strong correlation with conventional indices, its independent utility in guiding operability could not be established in this retrospective analysis. Prospective studies incorporating Cp into hemodynamic assessment and evaluating its association with clinical outcomes are required.
REFERENCES
- Lopes AA, Barst RJ, Haworth SG, Rabinovitch M, Dabbagh MA, Cerro MJ, Ivy D, Kashour T, Kumar K, Harikrishnan S, D'Alto M. Repair of congenital heart disease with associated pulmonary hypertension in children: what are the minimal investigative procedures? Consensus statement from the Congenital Heart Disease and Pediatric Task Forces, Pulmonary Vascular Research Institute (PVRI). Pulmonary Circulation. 2014;4(2):330-41. [Google Scholar] [PubMed]
- Van Der Feen DE, Bartelds B, de Boer RA, Berger RM. Assessment of reversibility in pulmonary arterial hypertension and congenital heart disease. Heart. 2019;105(4):276-82. [Crossref] [Google Scholar] [PubMed]
- Lopes AA, O’Leary PW. Measurement, interpretation and use of haemodynamic parameters in pulmonary hypertension associated with congenital cardiac disease. Cardiology in the young. 2009;19(5):431-5. [Crossref] [Google Scholar] [PubMed]
- Milnor WR, Jose AD, McGaff CJ. Pulmonary vascular volume, resistance, and compliance in man. Circulation. 1960;22(1):130-7. [Crossref] [Google Scholar] [PubMed]
- Basnet NB, Awa S, Hishi T, Yanagisawa M. Pulmonary arterial compliance in children with atrial and ventricular septal defect. Heart and vessels. 2000;15(2):61-9. [Crossref] [Google Scholar] [PubMed]
- Choubey M, Kothari SS, Gupta SK, Ramakrishnan S, Saxena A. Pulmonary arterial compliance in patients of CHD with increased pulmonary blood flow. Cardiology in the Young. 2023;33(10):1889-95. [Crossref] [Google Scholar] [PubMed]
- Mahapatra S, Nishimura RA, Sorajja P, Cha S, McGoon MD. Relationship of pulmonary arterial capacitance and mortality in idiopathic pulmonary arterial hypertension. Journal of the American College of Cardiology. 2006;47(4):799-803. [Crossref] [Google Scholar] [PubMed]
- LaFarge CG, Miettinen OS. The estimation of oxygen consumption. Cardiovascular research. 1970;4(1):23-30. [Crossref] [Google Scholar] [PubMed]
- Segers P, Brimioulle S, Stergiopulos N, Westerhof N, Naeije R, Maggiorini M, Verdonck P. Pulmonary arterial compliance in dogs and pigs: the three-element windkessel model revisited. American Journal of Physiology-Heart and Circulatory Physiology. 1999;277(2):H725-31. [Crossref] [Google Scholar] [PubMed]
- Stergiopulos N, Segers P, Westerhof N. Use of pulse pressure method for estimating total arterial compliance in vivo. American Journal of Physiology-Heart and Circulatory Physiology. 1999;276(2):H424-8. [Google Scholar] [PubMed]
- Ghio S, Schirinzi S, Pica S. Pulmonary arterial compliance: how and why should we measure it?. Global Cardiology Science and Practice. 2015;2015(4):58. [Crossref] [Google Scholar] [PubMed]
- Lopes AA, Barst RJ, Haworth SG, Rabinovitch M, Dabbagh MA, Cerro MJ, et al. Repair of congenital heart disease with associated pulmonary hypertension in children: what are the minimal investigative procedures? Consensus statement from the Congenital Heart Disease and Pediatric Task Forces, Pulmonary Vascular Research Institute (PVRI). Pulmonary Circulation. 2014;4(2):330-41. [Crossref] [Google Scholar] [PubMed]
- Muneuchi J, Nagatomo Y, Watanabe M, Joo K, Onzuka T, Ochiai Y, Joo K. Relationship between pulmonary arterial resistance and compliance among patients with pulmonary arterial hypertension and congenital heart disease. The Journal of Thoracic and Cardiovascular Surgery. 2016;152(2):507-13. [Crossref] [Google Scholar] [PubMed]
- Muneuchi J, Ochiai Y, Masaki N, Okada S, Iida C, Sugitani Y, et al. Pulmonary arterial compliance is a useful predictor of pulmonary vascular disease in congenital heart disease. Heart and Vessels. 2019;34(3):470-6. [Crossref] [Google Scholar] [PubMed]
- Thenappan T, Prins KW, Pritzker MR, Scandurra J, Volmers K, Weir EK. The critical role of pulmonary arterial compliance in pulmonary hypertension. Annals of the American Thoracic Society. 2016;13(2):276-84. [Crossref] [Google Scholar] [PubMed]
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 25-35 Days |
Peer Review Feedback |
| 45-60 Days | Total article processing time |
Ethics & Policies
Editorial & Management
Useful Links
Journal Highlights
Open Access Journals
Membership
Journal Flyer