Journal of Pediatric Medicine and Child Health
ISSN:
3108-2076 (Online)
DOI Prefix (Crossref): 10.67238
ABSTRACT
Background
Cancer remains a major public health challenge in India, where delayed detection is often linked to gaps in awareness and health-seeking behavior. Among tertiary students, understanding how individuals interpret cancer-related information and translate it into action is crucial. Although often discussed within the broader concept of health literacy, these processes are shaped by multiple psychosocial factors beyond knowledge.
Objective
This study examines cancer awareness and health-related behaviors among tertiary students in Punjab, India, focusing on how risk perception and related factors influence preventive actions and help-seeking.
Methods
A cross-sectional survey was conducted among tertiary students across selected districts in Punjab. Data were collected using a structured questionnaire that assessed cancer awareness, perceived risk, and health-promoting behaviors. Descriptive and inferential analyses were performed to examine the patterns and relationships among the variables.
Results
Awareness of cancer risk factors varied, with 65.6% of participants identifying smoking as a risk factor, while recognition of diet-related risks, such as obesity (26.1%) and red or processed meat (27.0%), was substantially lower. Awareness of warning signs was moderate, with fewer than half of the participants recognizing key symptoms such as unexplained weight loss and persistent cough. Engagement in health-promoting behaviors was inconsistent; for example, 42.4% of the participants reported adequate hydration, whereas only 25.6% engaged in regular physical activity. Cancer awareness was positively associated with health-promoting behavior (r = 0.559, p < .001), indicating that higher awareness was linked to better practices, although this did not translate into consistent behavior across all domains
Conclusion
The findings show that awareness contributes to health-promoting behaviors but does not consistently lead to sustained preventive action. Behavior appears to be influenced by a broader set of factors that affect knowledge application in daily life. Public health efforts should extend beyond awareness to support practical and contextually relevant behavior changes.
Keywords: Cancer Awareness; Health Behavior; Risk Perception; Tertiary Students; Public Health
INTRODUCTION
Cancer is one of the leading causes of morbidity and mortality worldwide. According to the Global Cancer Observatory, an estimated 19.3 million new cancer cases and nearly 10 million cancer-related deaths occurred globally in 2020, and the burden is expected to increase substantially over the coming decades because of population growth, aging, and changing exposure to risk factors [1]. Recent global cancer statistics further indicate that incidence rates continue to increase across many low- and middle-income countries, where healthcare systems often face challenges related to prevention, early diagnosis, and access to treatment [1].
India is experiencing a significant increase in the cancer burden. National estimates indicate that more than 1.4 million new cancer cases are diagnosed annually, with projections suggesting that the number may exceed 2 million cases by 2040 if current trends continue [2]. Lifestyle transitions, tobacco use, unhealthy dietary patterns, physical inactivity, environmental exposure, and population aging have all contributed to this increase [3]. Although advances in cancer diagnosis and treatment have improved survival outcomes in many settings, delayed presentation remains a major concern in India and other low- and middle-income countries, where many patients seek care only after symptoms become advanced [4].
Awareness of cancer risk factors, warning signs, and screening practices is considered essential for improving early detection and preventive behavior. Individuals who recognize symptoms and understand modifiable risk factors are generally more likely to seek timely medical attention and participate in preventive practices [5]. Nevertheless, evidence suggests that awareness alone does not necessarily translate into sustained health-promoting behavior or timely help-seeking. Several studies have shown that people may possess basic knowledge about cancer yet still avoid screening, delay reporting symptoms, or fail to adopt preventive lifestyles because of fear, fatalistic beliefs, stigma, low perceived susceptibility, or competing social and economic priorities [6].
These challenges are especially relevant in the Indian context, where social beliefs, cultural perceptions, and unequal access to health information influence how cancer is understood and discussed in society. Cancer is often associated with fear, suffering, social isolation, and death, which may discourage open communication and delay seeking healthcare. In some communities, misconceptions surrounding the causes of cancer and concerns about social judgment continue to shape attitudes toward people living with this disease. Such perceptions may contribute not only to delayed diagnosis but also to emotional distress and reduced social support for the affected individuals. This issue is particularly important among tertiary students. Young adults in universities and colleges represent an influential population because they are future professionals, community leaders, and decision-makers who may shape public attitudes and health practices over time. At the same time, this stage of life is often associated with the development of long-term behavioral patterns related to diet, physical activity, substance use, and healthcare utilization. Studies conducted among university students in different countries have reported uneven knowledge of cancer risk factors, limited awareness of screening practices, and inconsistent engagement in preventive behaviors despite relatively high educational attainment [7]. Similar concerns have been reported in Indian student populations, where awareness of certain cancers may be moderate, while understanding of warning signs and preventive practices remains limited.
These patterns are closely connected to the broader concept of health literacy, which refers to an individual’s ability to access, understand, evaluate, and apply health information to support informed decision-making. However, cancer-related behaviors are influenced by factors beyond knowledge alone. Psychological and social factors, such as perceived susceptibility, emotional responses, stigma, and social norms, play a significant role in shaping whether individuals act on health information or avoid it altogether [6,8]. The Health Belief Model further suggests that individuals are more likely to engage in preventive action when they perceive themselves to be at risk and believe that taking action will be beneficial [9]. Similarly, the Theory of Planned Behavior emphasizes the influence of attitudes, perceived social expectations, and behavioral control on health-related actions [10]. These perspectives help explain why awareness does not always lead to preventive behavior in practice.
Given these complexities, it is necessary to examine cancer awareness together with behavioral and psychosocial influences among young adults. This study, presented at the INZSOA-2-25:4th International North Zone Symposium of Anatomy on Integrative Approaches in Clinical Anatomy Bridging Genetics, Public Health and Nutrition, organized by Desh Bhagat Hospital and Dental College from February 27 and 28, 2025, investigates cancer awareness and health-promoting behavior among tertiary students in Punjab, India. The study explores how awareness relates to preventive behavior while also considering the influence of perceived risk and stigma on cancer-related attitudes and actions. By examining these interconnected factors, the study seeks to contribute to a clearer understanding of the challenges affecting cancer prevention and early help-seeking among young adults in the Indian context.
MATERIALS AND METHODS
Study Design
This study employed a cross-sectional quantitative design to examine cancer awareness and health-related behaviors among tertiary students in Punjab, India. The design allowed for the assessment of patterns and relationships between awareness, risk perception, and behavioral outcomes within a defined population at a single point in time.
Study Setting and Participants
The study was conducted across six districts in Punjab: Patiala, Mansa, Tarn Taran, Sangrur, Gurdaspur, and Shri Muktsar Sahib. These districts were selected to reflect regional diversity and variations in the cancer burden.
The participants were tertiary-level students enrolled in universities and colleges in these districts. The inclusion criteria were students aged 18-35 years enrolled in non-medical academic programs. Students from medical and health-related disciplines were excluded to minimize the influence of prior specialized knowledge of cancer awareness and perception. A multistage sampling approach was employed. In the first stage, the districts were purposively selected. In the second stage, institutions and student-accessible environments were approached based on feasibility. In the final stage, participants were recruited using convenience sampling across multiple settings, including campuses, hostels, libraries, and other student gathering areas.
The sample size was determined to ensure sufficient statistical power for estimating associations between cancer awareness, risk perception, stigma, and health-promoting behaviours among tertiary students. Given the large target population of approximately 503,322 tertiary students in Punjab (Ministry of Education, India, 2020), a finite population approach was used for sample size estimation. Based on the method proposed by Gill et al. (2010), a minimum sample size of 660 participants was required at a 95% confidence level with a 5% margin of error. To account for potential non-response, incomplete questionnaires, and data exclusions during cleaning, the target sample size was increased to 700 participants. After data cleaning, 601 fully completed questionnaires were retained for final analysis, yielding a response rate of 85.9%. This final sample size was considered adequate for conducting subgroup analyses and multivariate statistical testing.
Measures
Data were collected using a structured, self-administered questionnaire comprising validated instruments.
Cancer Awareness
Cancer awareness was assessed using the Cancer Awareness Measure (CAM), which evaluates knowledge of cancer risk factors, warning signs, and screening practices (Stubbings et al., 2009). Responses were aggregated to form a composite awareness score, with higher scores indicating greater awareness.
Risk Perception
Risk perception was measured using the Tripartite Model of Risk Perception (TRIRISK), which captures the deliberative (cognitive), affective (emotional), and experiential (intuitive) dimensions of perceived susceptibility to cancer [6]. Subscale and overall risk perception scores were computed.
Cancer-Related Stigma
Cancer-related stigma was assessed using selected items from the Cancer Stigma Scale (CASS), which examines beliefs, attitudes, and perceived social stigma associated with cancer.
Health-Promoting Behaviour
Health-promoting behavior was assessed using the Health-Promoting Lifestyle Profile II (HPLP-II), which measures engagement in behaviors such as physical activity, nutrition, stress management, and health responsibility. Higher scores reflect greater engagement in positive health practices.
Demographic Variables
Participants reported demographic information, including age, sex, district of residence, financial status, and family history of cancer.
Pilot Testing and Instrument Reliability
Prior to the main survey, a pilot study was conducted among 25 undergraduate students at Desh Bhagat University to assess the clarity, cultural appropriateness, and psychometric properties of the study instrument. Participants involved in the pilot study were excluded from the final sample. The pilot process evaluated item comprehension, response consistency, and survey flow, particularly for sensitive items related to cancer stigma and perceived cancer risk [11] recommended thresholds for psychosocial and health research instruments. Minor revisions were made following participant feedback to improve clarity and contextual relevance. For example, an item assessing comparative cancer risk perception was simplified to improve comprehension among respondents. Ambiguous or overly technical wording was revised to ensure better interpretability within the study population. Internal consistency reliability was assessed using Cronbach’s alpha coefficients, while temporal stability was evaluated using test-retest reliability. Reliability analyses demonstrated acceptable to excellent internal consistency across most scales, consistent with recommended thresholds for psychosocial and health research instruments [12,13]. The Cancer Stigma Scale demonstrated particularly strong reliability for the attitude-related items (α = .914), while the TRIRISK risk perception scale also showed excellent reliability (α = .864). Some subdomains within the Cancer Awareness Measure showed comparatively lower reliability and were interpreted cautiously in the final analysis. Table 1 displays the results of the reliability scores of the various scales used in this study.
|
Scale |
Subscale |
Cronbach’s Alpha |
Test-Retest Reliability (r) |
Interpretation |
|
Cancer Awareness Measure (CAM) |
Risk Factors |
0.819 |
0.989 |
Good |
|
Warning Signs |
0.594 |
0.858 |
Moderate |
|
|
Barriers to Help-Seeking |
0.504 |
0.928 |
Low |
|
|
TRIRISK Risk Perception Scale |
Total Scale |
0.864 |
0.995 |
Excellent |
|
Cancer Stigma Scale (CASS) |
Attitude Domain |
0.914 |
0.994 |
Excellent |
|
Feelings/Behaviour Domain |
0.636 |
0.985 |
Acceptable |
|
|
Health-Promoting Lifestyle Profile II (HPLP-II) |
Total Scale |
0.784 |
0.997 |
Good |
Table 1: Reliability Statistics for Study Instruments.
Note: Cronbach’s alpha values ≥ .70 indicate acceptable internal consistency [13].
The findings indicate that the study instrument demonstrated satisfactory psychometric performance and was suitable for assessing cancer awareness, stigma, risk perception, and health-related behaviours among tertiary students in Punjab.
Data Collection Procedure
Data were collected over three months following institutional approval. Trained research assistants administered the questionnaires in person across both academic and non-academic student settings, including campuses, hostels and common gathering spaces.
Participants were informed of the purpose of the study and provided written consent prior to participation. The questionnaires were completed anonymously to encourage honest responses, particularly for perception-related items. Research assistants were available to clarify questions where necessary, without influencing responses.
Completed questionnaires were checked for completeness, coded, and entered into a database using a double-entry process to minimize errors.
Data Analysis
Data were analyzed using IBM SPSS Statistics version 26. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize the levels of cancer awareness, risk perception, stigma, and health-related behavior.
Inferential analyses were conducted to examine the relationships between the variables. Independent samples t-tests were used to assess gender differences, while one-way analysis of variance was used to examine differences across demographic groups. Pearson’s correlation analysis was used to assess the relationships between awareness, risk perception, and behavior.
Multiple linear regression analysis was conducted to examine the predictors of risk perception, with cancer awareness, gender, age, financial status, and family history of cancer entered as independent variables. Statistical significance was set at P < 0.05.
Ethical Considerations
Ethical approval for the study was obtained from the Institutional Ethics Committee of Desh Bhagat University (Approval No. DBU/RC/2026/6406) prior to data collection. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki for research involving human participants [14].
Participation in the study was entirely voluntary. All participants received clear information regarding the purpose of the research, study procedures, confidentiality measures, and their right to withdraw at any stage without penalty. Written informed consent was obtained from all respondents before participation.
To protect participant privacy, questionnaires were completed anonymously, and no personally identifiable information was collected. All data were treated confidentially and used strictly for academic and research purposes. Access to the dataset was restricted to the research team, and all records were securely stored throughout the study period.
RESULTS
Demographic Characteristics
The demographic characteristics of the participants are shown in Table 2. A total of 601 tertiary students participated in the analysis. Of these, 324 (53.9%) were men and 277 (46.1%) were women. In terms of age distribution, the majority of participants were between 18 and 24 years (64.2%), followed by those aged 30–35 years (18.3%) and 25–29 years (17.5%).
Participants were drawn from six districts in Punjab, India. The highest proportion of respondents came from Patiala (19.6%) and Shri Muktsar Sahib (19.3%), followed by Mansa (17.3%), Sangrur (15.5%), Gurdaspur (15.1%), and Tarn Taran (13.1%) districts.
Regarding educational level, most participants were undergraduate students (58.9%), while 28.1% were postgraduate students. A smaller proportion was in other programs (11.8%), and only 1.2% were engaged in higher-level studies.
In terms of financial status, nearly half of the participants reported a middle-income background (49.6%), followed by middle-higher (36.9%), while smaller proportions reported low (6.7%) and higher (6.8%) financial statuses.
|
Variable |
Category |
n |
% |
|
Gender |
Male |
324 |
53.9 |
|
Female |
277 |
46.1 |
|
|
Age Group (years) |
18–24 |
386 |
64.2 |
|
25–29 |
105 |
17.5 |
|
|
30–35 |
110 |
18.3 |
|
|
District |
Patiala |
118 |
19.6 |
|
Shri Muktsar Sahib |
116 |
19.3 |
|
|
Mansa |
104 |
17.3 |
|
|
Sangrur |
93 |
15.5 |
|
|
Gurdaspur |
91 |
15.1 |
|
|
Tarn Taran |
79 |
13.1 |
|
|
Educational Level |
Undergraduate |
354 |
58.9 |
|
Postgraduate |
169 |
28.1 |
|
|
Higher |
7 |
1.2 |
|
|
Others |
71 |
11.8 |
|
|
Financial Status |
Low |
40 |
6.7 |
|
Middle |
298 |
49.6 |
|
|
Middle Higher |
222 |
36.9 |
|
|
Higher |
41 |
6.8 |
Table 2: Demographic Characteristics of Participants (N = 601)
Cancer Awareness
Awareness of Cancer Risk Factors
Participants’ awareness of cancer risk factors is shown in Table 3. Recognition varied across different risk factors. Lifestyle-related risks, such as smoking, were widely recognized, with 65.6% of respondents identifying them as cancer risk factors. Awareness was also relatively high for infections such as human papillomavirus (62.4%), family history of cancer (57.1%), and exposure to environmental and occupational toxins (55.8%).
Moderate levels of awareness were observed regarding secondhand smoke (57.6%), physical inactivity (54.7%), and ultraviolet radiation exposure (43.1%).
Lower levels of awareness were noted for alcohol consumption (40.3%) and low fruit and vegetable intakes (38.8%). Recognition was further reduced for red and processed meat (27.0%) and overweight or obesity (26.1%).
Older age was the least recognized risk factor, with only 19.0% of participants identifying it, while the majority either disagreed or were uncertain.
|
Risk Factor |
Disagree (%) |
Not Sure (%) |
Agree (%) |
|
Smoking |
29.8 |
4.5 |
65.6 |
|
Secondhand smoke |
28.6 |
13.8 |
57.6 |
|
Alcohol consumption |
34.6 |
25.1 |
40.3 |
|
Low fruit & vegetable intake |
31.3 |
30.0 |
38.8 |
|
Red/processed meat |
35.2 |
37.8 |
27.0 |
|
Overweight/obesity |
45.1 |
28.8 |
26.1 |
|
UV exposure |
29.3 |
27.6 |
43.1 |
|
Environmental toxins |
29.2 |
15.0 |
55.8 |
|
Infections (HPV, etc.) |
22.9 |
14.6 |
62.4 |
|
Family history |
23.4 |
19.5 |
57.1 |
|
Physical inactivity |
28.9 |
16.3 |
54.7 |
|
Older age (>70) |
57.6 |
23.5 |
19.0 |
Table 3: Awareness of Cancer Risk Factors Among Participants
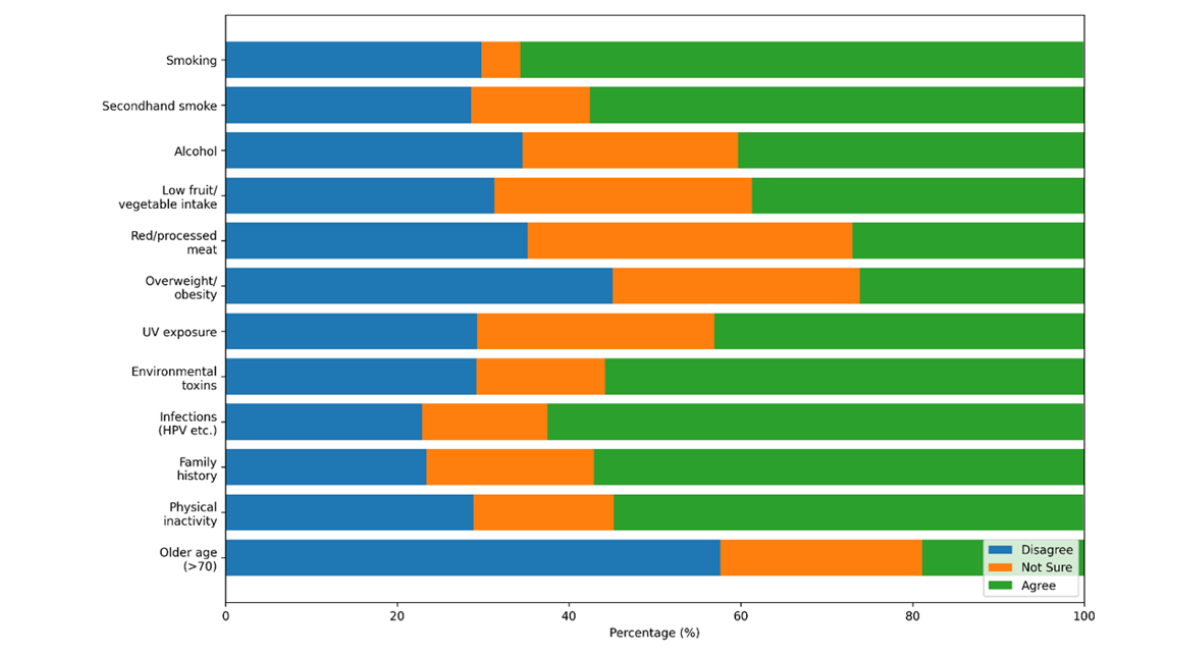
Figure 1: Awareness of Cancer Risk Factors among Participants
The figure illustrates participant responses regarding recognised cancer risk factors. Smoking (65.6%), infections such as HPV (62.4%), secondhand smoke (57.6%), and family history (57.1%) were the most commonly recognised risk factors. Awareness was lower for obesity (26.1%), red or processed meat consumption (27.0%), and older age (19.0%). Awareness varied substantially across cancer risk factors. Smoking, infections, family history, and secondhand smoke were recognised by most participants as cancer risks. In contrast, awareness was considerably lower for obesity, red and processed meat consumption, and older age, with large proportions of respondents either disagreeing or expressing uncertainty regarding these associations.
Awareness of Cancer Warning Signs
The awareness of cancer warning signs is presented in Table 4. Overall, symptom recognition was moderate, with no single warning sign identified by most participants.
The most common symptoms were persistent or worsening pain (53.9%), unexplained bleeding (46.8%), and changes in moles (46.6%). Other symptoms, including lumps or swelling (44.3%), bowel or bladder changes (44.3%), and persistent cough (43.4%), were identified by less than half of respondents.
A considerable proportion of participants either did not recognize or were uncertain about several symptoms. For instance, over 40% of respondents did not identify persistent pain or lumps as a warning sign. Uncertainty was highest for bowel or bladder changes (29.6%), breathing difficulty (26.0%), and unexplained weight loss (26.0%).
|
Warning Sign |
Yes (%) |
No (%) |
Don’t Know (%) |
|
Lump or swelling |
44.3 |
42.6 |
13.1 |
|
Persistent pain |
39.3 |
42.9 |
17.8 |
|
Unexplained bleeding |
46.8 |
30.3 |
23.0 |
|
Persistent cough |
43.4 |
33.1 |
23.5 |
|
Bowel or bladder changes |
44.3 |
26.1 |
29.6 |
|
Difficulty swallowing |
37.9 |
38.6 |
23.5 |
|
Change in mole |
46.6 |
31.4 |
22.0 |
|
Non-healing sore |
40.4 |
38.6 |
21.0 |
|
Persistent worsening pain |
53.9 |
27.3 |
18.8 |
|
Breathing difficulty |
40.1 |
33.9 |
26.0 |
|
Unexplained weight loss |
40.1 |
33.9 |
26.0 |
Table 4: Awareness of Cancer Warning Signs
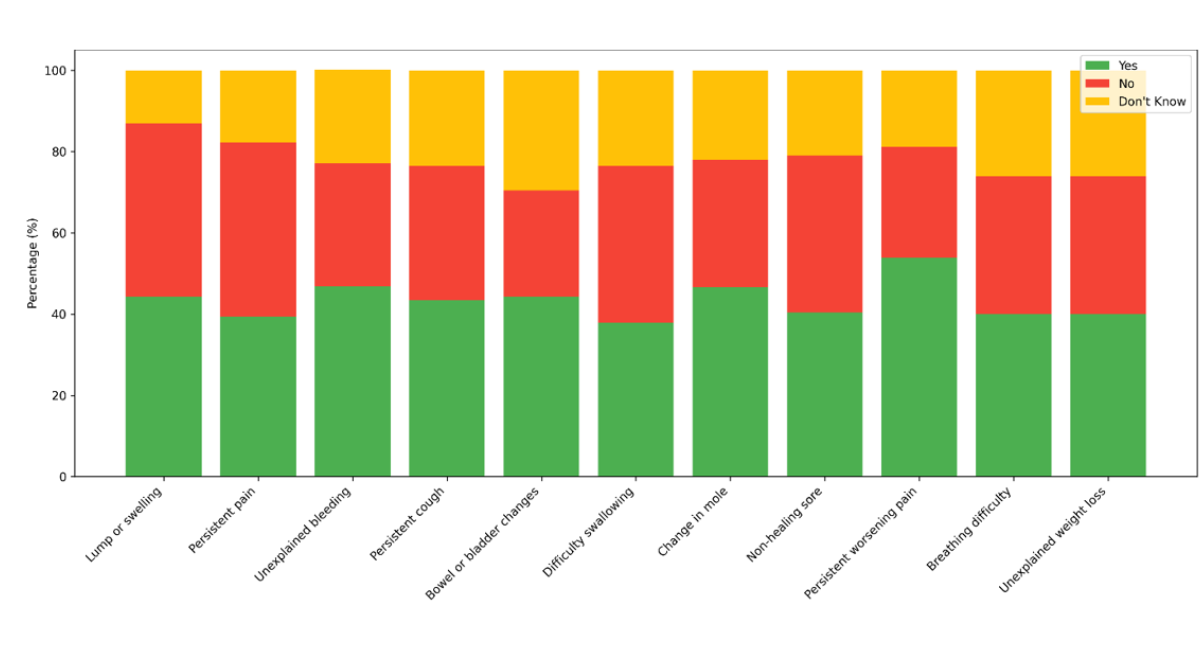
Figure 2: Awareness of Cancer Warning Signs among Participants (% Yes, No, and Don’t Know responses).
The stacked bar chart illustrates participants’ awareness of various cancer warning signs. Each bar represents a warning sign, divided into three segments showing the proportion of respondents who answered Yes, No, or Don’t Know. The chart highlights which signs, such as persistent worsening pain, are more widely recognized, and which signs, such as difficulty swallowing, show lower awareness, indicating potential areas for public health education.
Health-Promoting Behaviours
Health-promoting behaviors among the participants are presented in Table 5. Engagement in positive health practices varied across domains, with some behaviors more consistently adopted than others.
Dietary practices showed mixed patterns of association. A proportion of participants reported routinely consuming fruits and vegetables (28.6%) and maintaining adequate hydration (42.4%); however, many engaged in these behaviors only occasionally, indicating irregular adherence to recommended dietary habits. The physical activity levels were moderate. Approximately a quarter of the participants (25.6%) reported routine engagement in moderate exercise, while a notable proportion (22.6%) indicated that they never participated in such activities.
Preventive health behaviors also differed across practices. Participation in health screening programs was relatively high, with 37.4% of the participants reporting routine engagement. In contrast, reporting symptoms to health professionals was less consistent, with 27.3% of participants indicating that they never engaged in this behavior. Avoidance of major risk behaviors was more common. Most participants reported not using tobacco (60.9%) and limiting alcohol consumption (67.7%), although some individuals continued to engage in these behaviors.
Stress management and psychosocial behaviors showed some variability. Approximately one-third of the participants reported routinely getting enough sleep (31.9%), while behaviors such as seeking counselling or relying on social support were less consistently practised. These patterns suggest that although health-promoting behaviors are present among tertiary students, regular and sustained engagement remains uneven, indicating gaps between knowledge and everyday practice.
|
Behaviour |
Never (%) |
Sometimes (%) |
Often (%) |
Routinely (%) |
|
Eat 2–4 servings of fruits & vegetables |
12.1 |
36.1 |
23.1 |
28.6 |
|
Stay adequately hydrated |
18.8 |
21.1 |
17.6 |
42.4 |
|
Engage in moderate physical activity |
22.6 |
23.8 |
28 |
25.6 |
|
Participate in health screening programs |
16.3 |
25.1 |
21.1 |
37.4 |
|
Report symptoms to health professionals |
27.3 |
32.8 |
12.1 |
27.8 |
|
Avoid tobacco use |
60.9 |
18 |
16.8 |
4.3 |
|
Limit alcohol intake |
67.7 |
18.5 |
11.3 |
2.5 |
|
Get adequate sleep |
12.3 |
29.5 |
26.3 |
31.9 |
|
Seek guidance/counselling when needed |
14.8 |
31.6 |
33.4 |
20.1 |
|
Receive support from social networks |
26.5 |
23.8 |
25.8 |
24 |
Table 5: Selected Health-Promoting Behaviours Among Participants
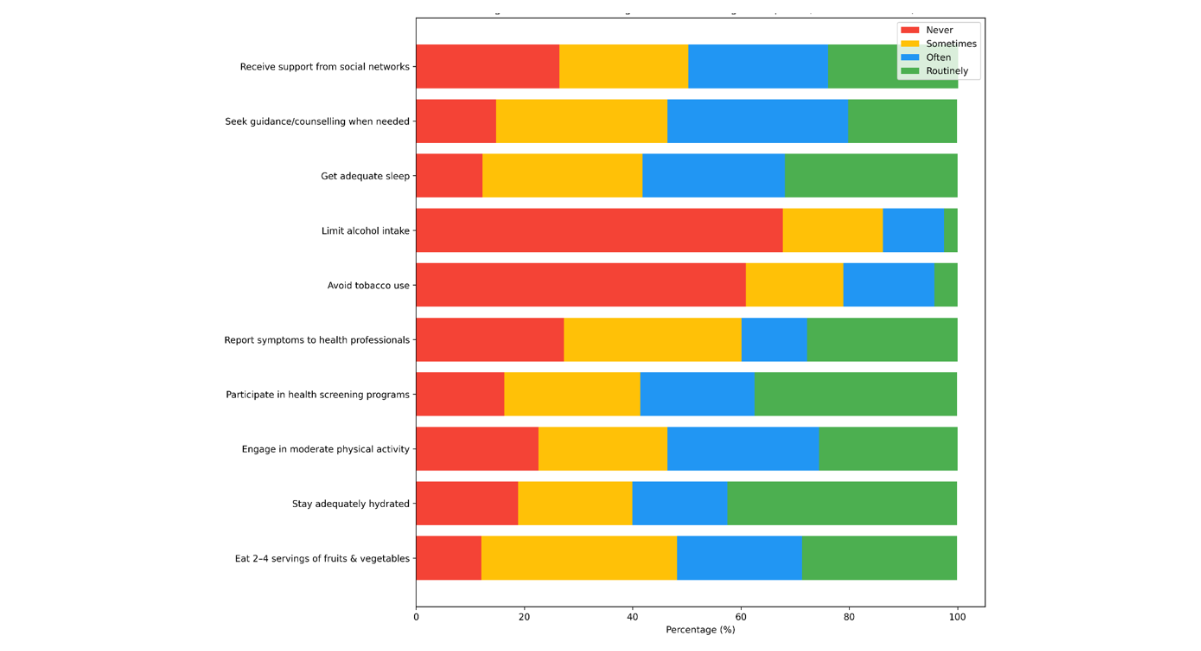
Figure 3: Engagement in Health-Promoting Behaviours among Participants (% Never, Sometimes, Often, and Routinely).
The horizontal stacked bar chart shows participants’ frequency of health-promoting behaviours. Each row represents a behaviour, and the segments indicate the proportion of participants who reported Never, Sometimes, Often, or Routinely engaging in it. This layout improves readability, especially for behaviours with long labels, and highlights patterns such as irregular dietary practices, moderate physical activity, and generally higher avoidance of risk behaviours like tobacco and alcohol use.
Gender Differences in Cancer Awareness, Risk Perception, Stigma, and Health-Promoting Behaviour
An independent samples t-test was conducted to examine gender differences in cancer awareness, risk perception, stigma, and health-promoting behavior among tertiary students. The findings are presented in Table 6.
Female respondents reported significantly higher cancer awareness scores (M = 140.67, SD = 15.76) than male respondents (M = 138.36, SD = 18.18), t = -2.23, p = .026. Female participants also demonstrated significantly higher levels of perceived cancer risk (M = 40.35, SD = 20.85) compared with males (M = 36.80, SD = 20.48), t = -2.00, p = .046.
In contrast, male respondents reported significantly higher stigma scores (M = 90.36, SD = 28.44) than female respondents (M = 82.38, SD = 28.18), t = 3.44, p = .001. This suggests that negative beliefs and stigmatizing attitudes toward cancer were more pronounced among males within the study population.
Health-promoting behaviour scores were also significantly higher among female respondents (M = 115.24, SD = 28.44) than males (M = 109.86, SD = 34.99), t = -2.04, p = .041. The findings indicate that female students were more likely to engage in preventive and health-supportive practices.
Taken together, the results suggest that gender differences exist across all four domains. Female respondents demonstrated higher awareness, greater perceived susceptibility, and stronger engagement in health-promoting behaviour, whereas male respondents exhibited higher levels of cancer-related stigma.
|
Variable |
Male Mean ± SD |
Female Mean ± SD |
t |
p |
|
Cancer awareness |
138.36 ± 18.18 |
140.67 ± 15.76 |
−2.23 |
.026 * |
|
Risk perception |
36.80 ± 20.48 |
40.35 ± 20.85 |
−2.00 |
.046 * |
|
Stigma |
90.36 ± 28.44 |
82.38 ± 28.18 |
3.44 |
.001 ** |
|
Health-promoting behaviour |
109.86 ± 34.99 |
115.24 ± 28.44 |
−2.04 |
.041 * |
Table 6: Gender Differences in Cancer Awareness, Risk Perception, Stigma, and Health-Promoting Behaviour.
Note: Independent samples t-test comparing male and female respondents. Higher scores indicate greater levels of the measured construct.
- p < .05, ** p < .01.
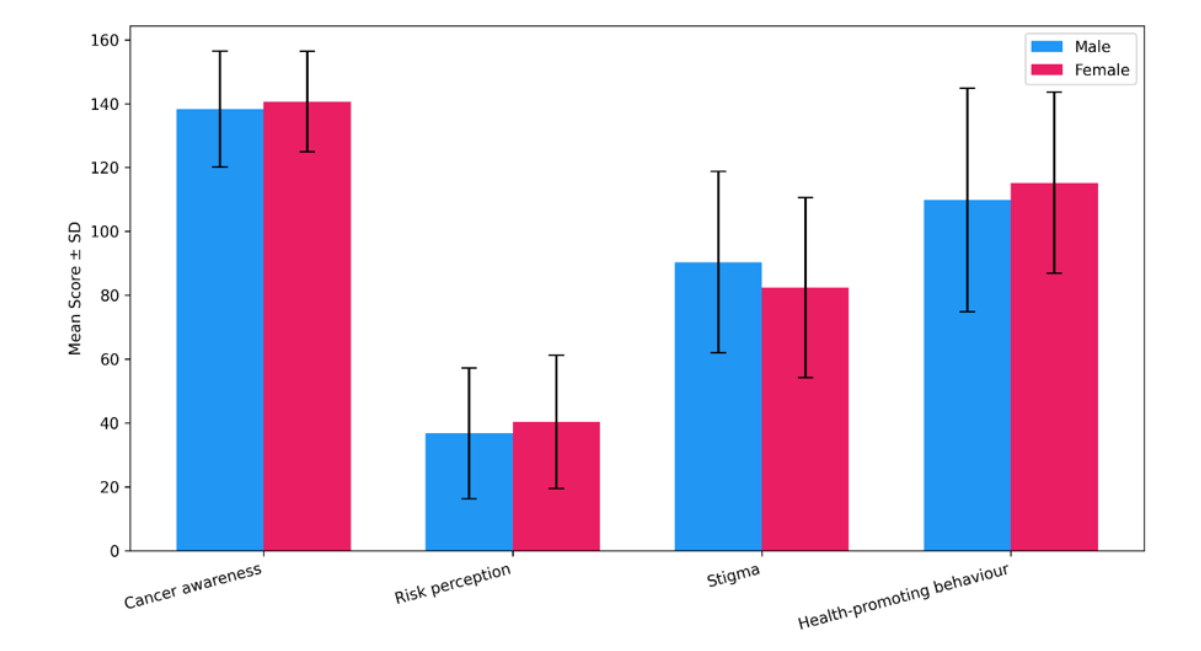
Figure 4: Comparison of Male and Female Participants’ Scores Across Cancer Awareness, Risk Perception, Stigma, and Health-Promoting Behavior (Mean ± SD).
The grouped bar chart illustrates gender differences across four domains. Female participants scored higher in cancer awareness, risk perception, and health-promoting behaviour, whereas males exhibited higher stigma scores. Error bars represent standard deviations, highlighting variability within each gender. This visualization makes the gender-based contrasts clear and emphasizes areas where interventions may be needed to reduce stigma and improve awareness among males.
Association among Cancer Awareness, Risk Perception, Stigma, and Health-Promoting Behaviors
Pearson’s correlation analysis was conducted to examine the relationship between cancer awareness and health-promoting behavior, as shown in Table 7. The results showed a moderate positive relationship between awareness and behavior (r = 0.559, p < .001), indicating that higher awareness was associated with increased engagement in health-promoting practices.
Risk perception was also positively correlated with health-promoting behavior (r = 0.547, p < .001), suggesting that individuals who perceive greater susceptibility are more likely to engage in preventive behaviors.
In contrast, stigma showed only a weak association with health behavior (r = 0.179, p < .001), indicating limited direct influence.
|
Variable |
Risk Perception |
Stigma |
Health-Promoting Behavior |
|
Cancer Awareness |
0.327 (< .001) *** |
0.111 (.006) ** |
0.559 (< .001) *** |
|
Risk Perception |
- |
−0.084 (.040) * |
0.547 (< .001) *** |
|
Stigma |
- |
- |
179) |
Table 7: Pearson Correlation Matrix of Cancer Awareness, Risk Perception, Stigma, and Health-Promoting Behaviors
DISCUSSION
This study examined cancer awareness and health-promoting behaviors among tertiary students in Punjab, India, with particular attention to how awareness translates into preventive action. The findings show that although awareness, risk perception, and health-promoting behavior were significantly associated, knowledge alone did not consistently result in sustained preventive practices. The study also highlights important psychosocial and behavioral gaps that may influence cancer prevention among young adults.
Awareness of cancer risk factors varied considerably across domains. Participants demonstrated stronger awareness of highly publicized risk factors, such as smoking, infections, and family history, whereas awareness of obesity, processed meat consumption, physical inactivity, and older age as cancer risk factors was substantially lower. This pattern reflects trends reported in both Indian and international literature. Studies conducted among university students and young adults have consistently shown greater recognition of tobacco-related risks than lifestyle and metabolic risk factors [5]. Similar findings have been reported in population-based research across Europe and Asia, where awareness is often influenced by the visibility of public health campaigns rather than a comprehensive understanding of cancer prevention [4].
Recognition of cancer warning signs was inconsistent. Although some symptoms were moderately identified, uncertainty remained substantial for several early warning indicators. Poor symptom awareness has important implications because delayed recognition is closely linked to delayed help-seeking and late-stage diagnosis [4]. Research from low- and middle-income settings has repeatedly demonstrated that limited symptom awareness contributes to poorer cancer outcomes, especially among younger populations who may underestimate their personal susceptibility to disease.
The findings relating to health-promoting behavior revealed a similar uneven pattern. Some participants reported positive practices, such as adequate hydration, moderate fruit and vegetable intake, and avoidance of tobacco or alcohol use. However, engagement in regular physical activity, dietary regulation, routine screening, and proactive health seeking remained inconsistent. Comparable findings have been observed among university students in several countries, where awareness of healthy lifestyles does not necessarily translate into sustained preventive behavior [7]. Studies among Indian tertiary students have also reported that academic stress, irregular schedules, sedentary routines, and limited access to preventive services often interfere with healthy behavioral practices despite moderate awareness levels [15].
Correlation analysis provides additional insights into these behavioral patterns. Cancer awareness was moderately positively associated with health-promoting behavior, indicating that respondents with higher awareness were more likely to engage in preventive practices. Risk perception also showed a significant positive relationship with health-promoting behavior, suggesting that students who perceived themselves to be vulnerable to cancer were more inclined toward healthier actions. These findings align with evidence from behavioral and public health research showing that awareness and perceived susceptibility are important predictors of preventive behavior and screening uptake [6]. At the same time, the moderate strength of these associations suggests that awareness and perceived risk explain only part of the behavioral variation observed in the study population.
The gender differences identified in this study are noteworthy. Female respondents demonstrated significantly higher levels of cancer awareness, greater perceived susceptibility, and stronger engagement in health-promoting behaviors, whereas male respondents reported higher stigma scores. Similar patterns have been documented internationally, wherein women tend to demonstrate stronger preventive health orientations and greater utilization of health services than men [14]. Higher stigma scores among male participants may reflect broader social and cultural expectations surrounding masculinity, emotional expression, and help-seeking behavior, factors that have been associated with poorer preventive health practices in previous studies [9].
The persistence of inconsistent behaviors despite moderate awareness and perceived risk highlights the influence of psychosocial and contextual factors. This pattern is consistent with the Health Belief Model, which proposes that awareness alone may not lead to preventive action unless individuals perceive themselves to be personally susceptible and believe that the benefits of action outweigh perceived barriers [10]. Similarly, the Theory of planned behavior suggests that attitudes, perceived social expectations, and behavioral control influence whether knowledge is translated into action. These findings also reflect the principles of social cognitive Theory, which emphasizes that behavior is influenced by the interaction between personal beliefs, social environment, and behavioral experiences [15]. Fear of diagnosis, cancer-related stigma, anad emotional avoidance may discourage young adults from translating awareness into action. Evidence from psycho-oncology research has shown that stigma and fear can significantly reduce participation in screening, disclosure, and timely help-seeking, even among individuals with adequate knowledge about cancer [16].
These findings have important implications for cancer prevention efforts in educational settings. Although awareness campaigns remain important, information alone is unlikely to produce sustained behavioral change. Preventive strategies should also address emotional barriers, stigma, institutional support, and practical access to health services. Educational institutions may play an important role by integrating cancer education into student wellness programs, expanding access to counselling and screening opportunities, and promoting supportive peer environments. Evidence from university-based health promotion programs suggests that interventions combining education with environmental and behavioral support are more effective than awareness-only approaches in improving preventive health practices among young adults [17].
This study has several strengths. The relatively large sample size and inclusion of participants from multiple districts improve the relevance of the findings within the Punjab context. The study also examined awareness alongside psychosocial and behavioral dimensions, providing a broader understanding of cancer-related behavior among tertiary students [18]. However, certain limitations should be acknowledged. The cross-sectional design limits causal interpretation, and the reliance on self-reported data introduces the possibility of recall bias and social desirability bias. In addition, although most study scales demonstrated acceptable to excellent reliability, some subscales within the Cancer Awareness Measure showed lower internal consistency, particularly the warning signs and barriers to help-seeking domains. These lower Cronbach’s alpha values suggest that findings related to these subscales should be interpreted cautiously and may require further refinement and validation in future studies. The pilot sample size was also relatively small, although it was sufficient for preliminary instrument refinement and reliability assessment [19-23].
The findings indicate that awareness and perceived risk contribute to health-promoting behavior; however, they do not fully explain how individuals respond to cancer-related information. Preventive action appears to depend on a wider set of emotional, social, and contextual influences [24,25]. Strengthening cancer prevention among young adults therefore requires approaches that move beyond awareness alone and address the broader conditions that shape health behavior.
CONCLUSION
This study examined cancer awareness, risk perception, stigma, and health-promoting behavior among tertiary students in Punjab, India. The findings show that awareness of cancer risk factors and warning signs was uneven across domains. Participants demonstrated stronger awareness of highly publicized risks, such as smoking and infections, whereas awareness of lifestyle-related and metabolic risk factors was considerably lower. Recognition of several warning signs was also inconsistent, indicating important gaps in cancer-related knowledge among young adults.
The study further revealed that awareness did not consistently translate into preventive behavior. Although some participants reported positive health practices, including avoidance of tobacco and moderate dietary habits, engagement in regular physical activity, proactive health seeking, and preventive practices remained inconsistent. Significant associations between awareness, risk perception, and health-promoting behavior suggest that these factors influence preventive action; however, they do not fully explain behavioral patterns among students.
Gender differences were also evident. Female respondents demonstrated higher levels of awareness, greater perceived susceptibility to cancer, and stronger engagement in health-promoting behaviors, whereas male respondents reported higher stigma scores. These findings suggest that social and psychosocial factors may shape how young adults perceive cancer and respond to health-related information.
The findings also highlight the continuing influence of stigma and emotional barriers. Fear, discomfort, and misconceptions surrounding cancer may discourage open discussion, delay help seeking, and limit engagement in preventive practices. Cancer prevention among young adults therefore requires more than awareness-raising alone. Educational and public health interventions should also address stigma, emotional responses, institutional support, and practical access to preventive services.
Despite certain limitations, including the cross-sectional design and lower reliability scores in some awareness subscales, this study provides important evidence on cancer-related perceptions and behaviors among tertiary students in Punjab. The findings underscore the need for context-sensitive and behavior-focused approaches that strengthen not only awareness but also the practical conditions that support healthier choices and earlier engagement with cancer prevention and care.
CONFLICT OF INTEREST
The authors declare no conflict of interest
FUNDING
This study received no funding from any agency or individuals
REFERENCES
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel R, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. [Crossref] [Google Scholar] [PubMed]
- Mathur P, Sathishkumar K, Chaturvedi M, Das P, Sudarshan KL, Santhappan S, et al. Cancer statistics, 2020: report from national cancer registry programme, India. JCO Glob Oncol. 2020;6:1063-1075. [Crossref] [Google Scholar] [PubMed]
- World Health Organization. Cancer country profiles 2023: India. 2023.
- Forbes LJ, Simon AE, Warburton F, Boniface D, Brain KE, Dessaix A, et al. Differences in cancer awareness and beliefs between Australia, Canada, Denmark, Norway, Sweden and the UK (the International Cancer Benchmarking Partnership): do they contribute to differences in cancer survival?. Br J Cancer. 2013;108(2):292-300. [Crossref] [Google Scholar] [PubMed]
- Marlow LA, Wardle J, Waller J. Understanding cervical screening non-attendance among ethnic minority women in England. Br. J. Cancer. 2015;113(5):833-839.[Crossref] [Google Scholar] [PubMed]
- Ferrer RA, Klein WM, Persoskie A, Avishai-Yitshak A, Sheeran P. The tripartite model of risk perception (TRIRISK): Distinguishing deliberative, affective, and experiential components of perceived risk. Ann Behav Med. 2016;50(5):653-663. [Crossref] [Google Scholar] [PubMed]
- Pengpid S, Peltzer K, Kassean HK, Tsala JP, Sychareun V, Müller-Riemenschneider F. Physical inactivity and associated factors among university students in 23 low-, middle-and high-income countries. Int. J. Public Health. 2015;60(5):539-549. [Crossref] [Google Scholar] [PubMed]
- Kline RB. Principles and practice of structural equation modeling. Guilford publications. 2023. [Google Scholar]
- Rosenstock IM. Historical origins of the health belief model. Health Educ. Monogr. 1974;2(4):328-335. [Crossref] [Google Scholar] [PubMed]
- Ajzen I. The Theory of planned behavior. Org. Behav. Hum. Decis. Process. 1991. [Crossref] [Google Scholar]
- Taber, K. S. (2018). The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ, 48(6), 1273-1296. [Crossref] [Google Scholar]
- Devellis RF, Thorpe CT. Scale development: Theory and applications. Sage publications; 2021. [Google Scholar]
- Bandura A. Social foundations of thought and action. Englewood Cliffs NJ. 1986;23-28:2. [Google Scholar]
- Champion VL, Skinner CS. The health belief model. Health behavior and health education: Theory, research, and practice. 2008;4:45-65. [Google Scholar]
- Glanz K, Rimer BK, Viswanath K. Health behavior: Theory, research, and practice. John Wiley & Sons; 2015. [Google Scholar]
- Menon U, Szalacha L, Prabhughate A, Kue J. Correlates of colorectal cancer screening among South Asian immigrants in the United States. Cancer Nurs. 2014;37(1):E19-27. [Crossref] [Google Scholar] [PubMed]
- Moser RP, Mccaul K, Peters E, Nelson W, Marcus SE. Associations of perceived risk and worry with cancer health-protective actions: data from the Health Information National Trends Survey (HINTS). J. Health Psychol. 2007;12(1):53-65. [Crossref] [Google Scholar] [PubMed]
- Mushini V, Chandra PS, Rao R, Raj S, Piang LK, Nair KS, et al. Awareness regarding risk factors, symptoms and treatment facilities for cancer in selected states of India. Asian Pacific Journal of Cancer Prevention. 2012;13(8):4057-4062. [Crossref] [Google Scholar] [PubMed]
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. [Crossref] [Google Scholar] [PubMed]
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021;71(3):209-249. [Crossref] [Google Scholar] [PubMed]
- Stubbings S, Robb K, Waller J, Ramirez A, Austoker J, Macleod U, et al. Development of a measurement tool to assess public awareness of cancer. Br. J. Cancer. 2009;101(2):S13-S17. [Crossref] [Google Scholar] [PubMed]
- Vrinten C, Gallagher A, Waller J, Marlow LA. Cancer stigma and cancer screening attendance: a population based survey in England. BMC cancer. 2019;19(1):566. [Crossref] [Google Scholar] [PubMed]
- World Health Organization. Guide to cancer early diagnosis. 2020.
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. Jama. 2013;310(20):2191-2194. [Crossref] [Google Scholar] [PubMed]
- Vernon SW. Risk perception and risk communication for cancer screening behaviors: a review. JNCI Monographs. 1999;1999(25):101-109. [Crossref] [Google Scholar] [PubMed]
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 25-35 Days |
Peer Review Feedback |
| 45-60 Days | Total article processing time |
Journal Flyer