Journal of Cardiology and Heart Failure
ISSN:
3139-6429 (Online)
DOI Prefix (Crossref): 10.67238
ABSTRACT
Background
Percutaneous Coronary Intervention (PCI) for Chronic Total Occlusions (CTO) is technically demanding. Even lesions with favorable angiographic characteristics may behave unpredictably and require strategic adaptation.
Case Summary
A 55-year-old male with Canadian Cardiovascular Society (CCS) class II–III angina was found to have a short, tapered chronic total occlusion of the mid-right coronary artery (RCA) at the level of the right ventricular (RV) branch. Initial antegrade wiring with an Asahi XTA wire crossed the occlusion but entered a side branch, resulting in extensive subintimal dissection. Subsequent antegrade dissection re-entry (ADR) and parallel-wire attempts failed and were complicated by distal tip fracture of a Caravel microcatheter. After a strategic pause and administration of intracoronary nitroglycerin, repeat angiography revealed a clearly visualized true lumen channel distal to the bifurcation. A dual-lumen microcatheter (Crusher double-lumen microcatheter, Boston Scientific) successfully redirected the guidewire into the distal true lumen, allowing completion of PCI using a double kissing crush (DKC) technique with restoration of TIMI-3 flow.
Keywords: Chronic Total Occlusion; Percutaneous Coronary Intervention; Double-Lumen Microcatheter; Subintimal Dissection; Microcatheter Fracture; Bifurcation PCI
INTRODUCTION
Chronic total occlusions (CTOs), defined as complete coronary artery occlusions of ≥3 months duration, represent one of the most complex challenges in interventional cardiology [1]. Although CTO PCI requires meticulous planning and advanced technical expertise, it remains associated with higher complication rates compared with non-CTO PCI [2]. Procedural complexity is multifactorial, involving lesion length, calcification, tortuosity, and the potential for complications such as distal dissection and equipment failure [3].
This case report describes a short RCA CTO that evolved into a complex procedural scenario involving subintimal dissection and microcatheter tip fracture. It emphasizes procedural adaptability, strategic escalation, and the pivotal role of a double-lumen microcatheter in achieving success after failure of conventional techniques.
CASE PRESENTATION
A 55-year-old hypertensive, non-diabetic male presented with CCS class II–III angina despite optimal medical therapy. Non-invasive stress testing demonstrated inferior wall ischemia. Transthoracic echocardiography showed preserved left ventricular systolic function without regional wall motion abnormalities.
Diagnostic coronary angiography revealed mild non-obstructive disease in the left anterior descending (LAD) and left circumflex (LCX) arteries. The mid-RCA demonstrated a very short but heavily calcified CTO located at the level of the right ventricular (RV) branch, with both antegrade and retrograde collateral filling (Figure 1). Given persistent symptoms, objective ischemia, and suitable distal vessel target, CTO PCI was deemed appropriate.
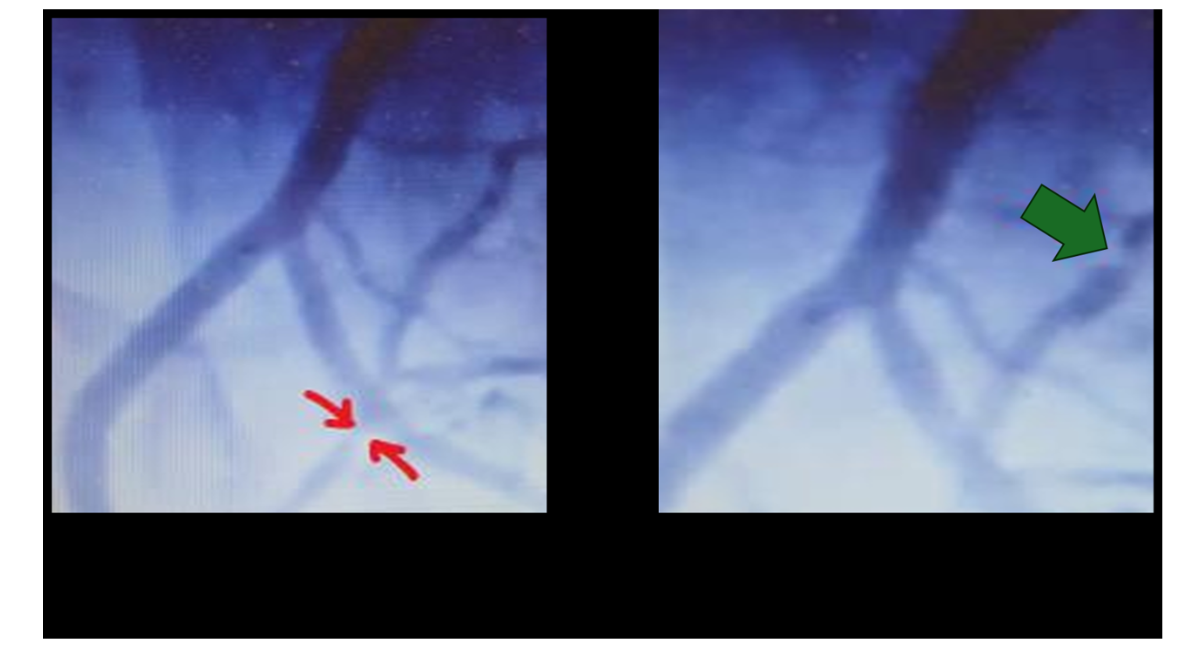
Figure 1: Initial angiography showing CTO of the RCA, red arrow: distal RCA occlusion, green arrow: Posterior Descending Artery (PDA) occlusion.
Procedural Course and Challenges
Radial access was obtained, and the RCA was engaged using a 7-Fr guide catheter. Lesion complexity was assessed using the Chinese CTO (CH-CTO) score, suggesting high procedural difficulty despite the short occlusion length.
Initial antegrade wiring with an Asahi XTR failed to cross the occlusion. A supported attempt using a Caravel microcatheter and an Asahi XTA wire allowed advancement across the occlusion; however, contrast injection demonstrated entry into a false lumen with extensive RCA dissection beyond the bifurcation and preferential filling of a distal side branch (Figure 2).
Given the subintimal position, antegrade dissection re-entry (ADR) was attempted. Despite anchor support, the microcatheter remained uncrossable, resulting in ADR failure.

Figure 2: Dissection of the RCA beyond the bifurcation
Microcatheter Tip Fracture and Retrieval Attempts
During withdrawal of the Caravel microcatheter to initiate a parallel-wire strategy, distal tip fracture was identified (Figure 3).
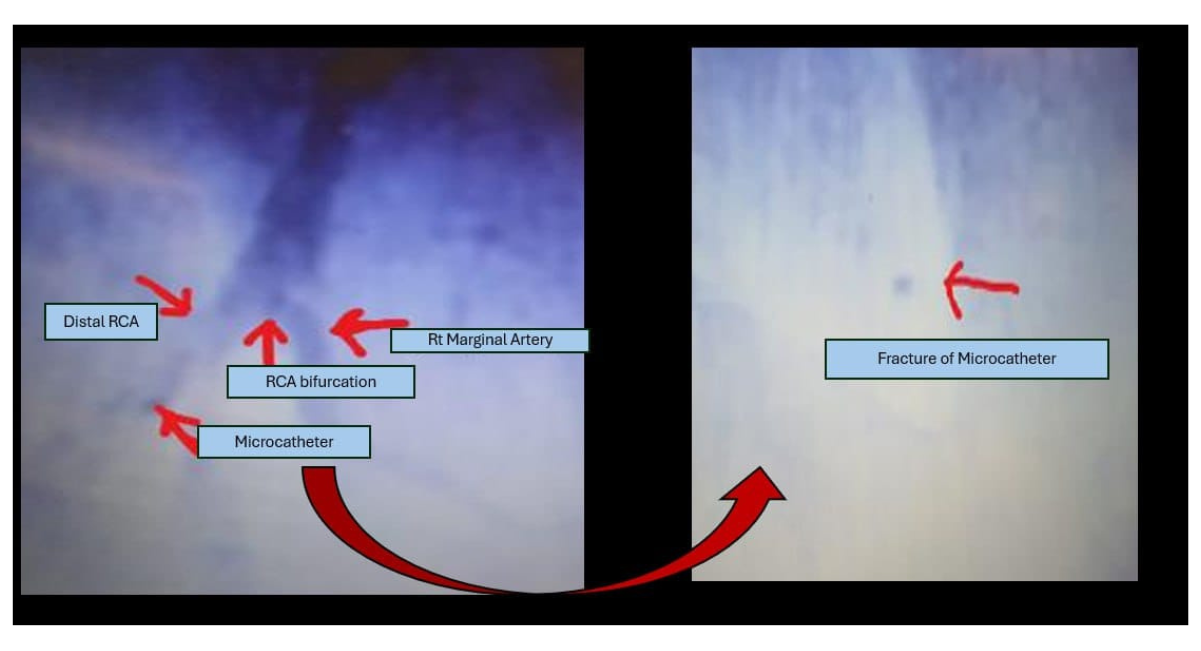
Figure 3: Tip fracture of the microcatheter
Multiple retrieval attempts were performed using a 1.5-mm balloon inflated at low pressure, positioned both proximal and distal to the retained fragment; however, these attempts failed to retrieve or dislodge the segment (Figure 4).
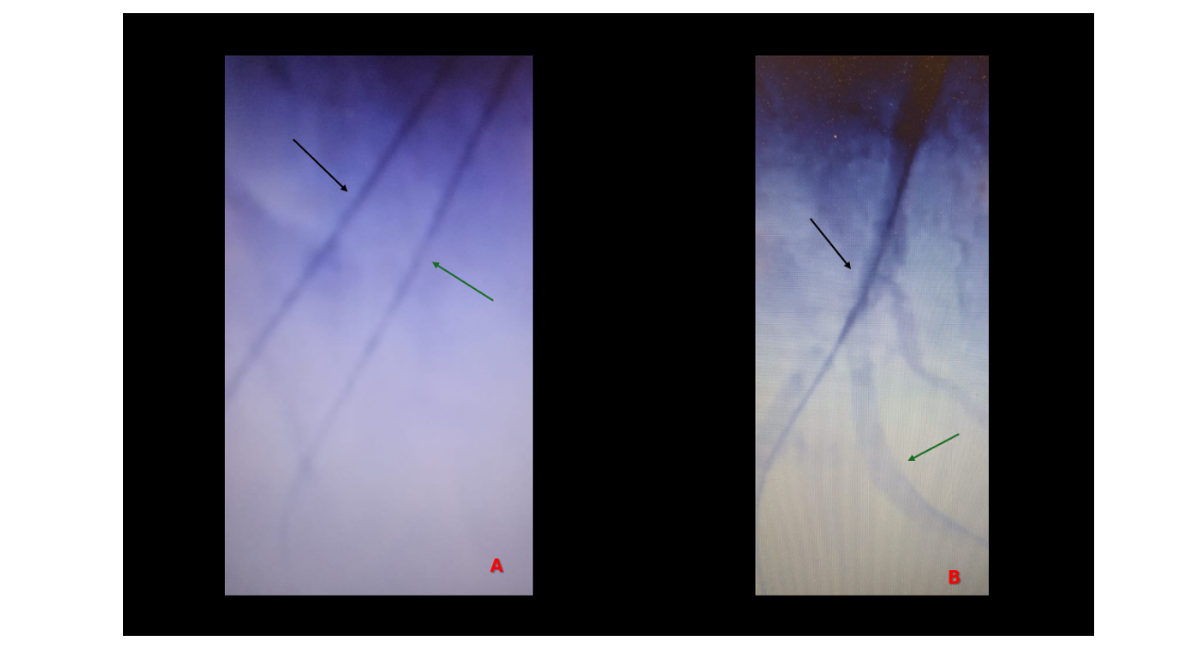
Figure 4: black arrow: wire 1, green arrow: wire 2, A: Parallel wire technique, B: Healthy track just after the RCA bifurcation
Subsequent parallel-wire attempts repeatedly entered the same false lumen. A knuckled Asahi XTA wire was then used in an attempt to recross the lesion, but re-entry into the distal true lumen was unsuccessful. At this stage—following failed ADR, failed parallel-wire attempts, and unsuccessful recrossing—the procedure was nearly aborted in favor of an investment strategy (Figure 4A).
Strategic Reassessment and Turning Point
All equipment was removed, and intracoronary nitroglycerin was administered. Repeat angiography unexpectedly demonstrated a clearly visualized true lumen channel distal to the bifurcation (Figure 4B), likely unmasked after resolution of vasospasm or extraluminal contrast staining.
Encouraged by this finding, a final attempt was undertaken using a torquable dual-lumen microcatheter (Twin-Pass / Crusher type). Through the second lumen, an Asahi XTA wire was manipulated and successfully directed into the distal true lumen on the first attempt.
Final Strategy and Procedural Success
Following successful wire positioning, the lesion was prepared with balloon pre-dilatation. PCI was completed using a double kissing crush (DKC) technique to treat the bifurcation involving the RCA and the RV branch. Final angiography demonstrated optimal stent expansion with complete restoration of TIMI-3 flow (Figure 5).
The patient remained hemodynamically stable without periprocedural complications. He was discharged on dual antiplatelet therapy and guideline-directed medical therapy. At three-month follow-up, he reported complete resolution of anginal symptoms without adverse cardiovascular events
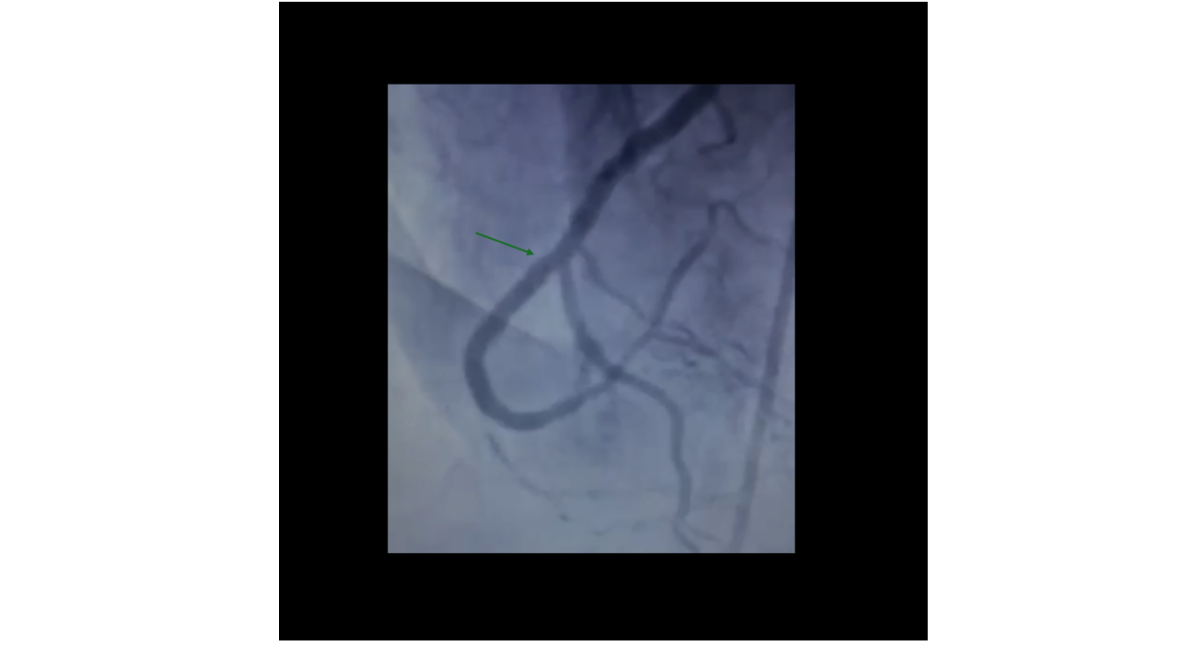
Figure 5: Final angiographic result after DKC technique
DISCUSSION
This case illustrates how an anatomically “favorable” chronic total occlusion (CTO) can evolve into an unexpectedly challenging intervention. Despite the lesion’s short length and tapered morphology—features typically associated with higher success in J-CTO and PROGRESS CTO scores—the procedure deviated rapidly from the anticipated course.
Registry data, including the prospective TOAST-GISE study, demonstrate lower technical success rates in the presence of long occlusions, moderate-to-severe calcification, or multivessel disease [4]. A large meta-analysis similarly identified vessel tortuosity, blunt stump morphology, and severe calcification as strong negative predictors of success [5]. In the present case, although several classical high-risk features were absent, involvement of the RV branch at a bifurcation introduced a critical layer of complexity. This aligns with literature emphasizing that side-branch involvement and bifurcation anatomy can significantly reduce crossing success, causing a seemingly low-risk lesion to behave as a high-risk one [4,5].
The subsequent failure to re-enter the true lumen and the occurrence of microcatheter tip fracture further escalated procedural difficulty. Device-related issues, particularly microcatheter damage or entrapment, are recognized but relatively uncommon complications in CTO PCI and may increase the risk of adverse events or procedural abandonment [5]. However, most published reports focus primarily on retrieval techniques rather than successful procedural continuation following fracture. In this context, our case stands out by demonstrating that successful revascularization can still be achieved within the same session despite confirmed distal tip fracture and failed re-entry attempts.
Ultimately, procedural success depended on strategic adaptation rather than additional force. Current evidence and expert consensus support escalation to advanced devices, including dual-lumen microcatheters and dedicated re-entry systems, when initial antegrade attempts fail [6]. In this case, after a deliberate pause and reassessment, introduction of a double-lumen microcatheter proved decisive. This reinforces that operator judgment, timely device escalation, and intraprocedural reassessment may be more determinative of outcome than pre-procedural scoring systems alone.
In summary, CTO PCI is a dynamic process in which intraprocedural developments frequently dictate strategy. Favorable angiographic characteristics do not guarantee procedural simplicity, and adaptability remains central to achieving technical success.
Key Clinical Lessons
- Short, tapered CTOs may become highly complex when bifurcation anatomy is involved.
- Microcatheter tip fracture does not necessarily mandate procedural abandonment if distal vessel integrity is preserved.
- A strategic pause with reassessment can significantly alter procedural trajectory.
- Escalation of strategy—not force—should guide CTO intervention.
- Dual-lumen microcatheters provide controlled wire redirection after failed antegrade techniques.
CONCLUSION
CTO PCI represents a dynamic interplay between pre-procedural planning and intraprocedural adaptability. Favorable angiographic features do not guarantee procedural ease. When unexpected complications arise—particularly bifurcation involvement and device-related failure—strategic reassessment and timely escalation to specialized tools can transform a near-failed intervention into a successful outcome.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
CONFLICTS OF INTEREST / COMPETING INTERESTS
The author(s) declare that they have no competing interests.
ETHICS APPROVAL
Ethical approval was obtained in accordance with institutional requirements. Verbal ethical approval was obtained from the patient prior to participation.
CONSENT TO PARTICIPATE
Verbal informed consent to participate in this study was obtained from the patient.
CONSENT FOR PUBLICATION
Verbal informed consent for publication of the patient’s data was obtained from the patient.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
CODE AVAILABILITY
Not applicable. No software application or custom code was used or generated in this study.
AUTHORS’ CONTRIBUTIONS
SA introduced the case, supervised it, and did the investigations, and methods. LA, JM, and NAH wrote the manuscript, collected the resources, and reviewed the manuscript.
PATIENT AND PUBLIC INVOLVEMENT
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
DISCLAIMER
The views expressed in this article are those of the author(s) and do not necessarily reflect the official position or policy of the affiliated institution or any funding body.
REFERENCES
- Di Mario C, Werner GS, Sianos G, Galassi AR, Büttner J, Dudek D et al. European perspective in the recanalisation of Chronic Total Occlusions (CTO): consensus document from the EuroCTO Club. EuroIntervention: journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology. 2007;3(1):30-43. [Google Scholar] [PubMed]
- Fefer P, Knudtson ML, Cheema AN, Galbraith PD, Osherov AB, Yalonetsky S, et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol. 2012;59(11):991-7. [Crossref] [Google Scholar] [PubMed]
- Galassi AR, Werner GS, Boukhris M, Azzalini L, Mashayekhi K, Carlino M, et al. Percutaneous recanalization of chronic total occlusions: 2019 Consensus. EIJ-D-18-00826; 2014. [Crossref] [Google Scholar] [PubMed]
- Olivari Z, Rubartelli P, Piscione F, Ettori F, Fontanelli A, Salemme L, et al . Immediate results and one-year clinical outcome after percutaneous coronary interventions in chronic total occlusions: data from a multicenter, prospective, observational study (TOAST-GISE). J Am Coll Cardiol. 2003;41(10):1672-8. [Crossref] [Google Scholar] [PubMed]
- Wang N, Fulcher J, Abeysuriya N, Adams M, Lal S. Predictors of successful chronic total occlusion percutaneous coronary interventions: a systematic review and meta-analysis. Heart. 2018;104(6):517-24. [Crossref] [Google Scholar] [PubMed]
- Mehta AB, Mehta N, Chhabria R, Mandurke V, Tawade N, Jain N, et al. Predictors of success in percutaneous Coronary intervention for chronic total occlusion. Indian Heart J. 2018;70:S269-74. [Crossref] [Google Scholar] [PubMed]
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 25-35 Days |
Peer Review Feedback |
| 45-60 Days | Total article processing time |
Ethics & Policies
Editorial & Management
Useful Links
Journal Highlights
Open Access Journals
Membership
Journal Flyer