Journal of Cardiology and Heart Failure
ABSTRACT
A 50-year-old elite marathon runner with a remarkable family history of sudden cardiac death (SCD) presented with brief episodes of burning chest discomfort occurring during warm-up and resolving with continued exertion. Despite exceptional physical fitness and absence of traditional cardiovascular risk factors, coronary computed tomography angiography (CCTA) revealed significant multivessel coronary artery disease involving the left anterior descending (LAD), left circumflex (LCx), and right coronary artery (RCA). Invasive coronary angiography confirmed severe stenoses. The calculated SYNTAX score was 18 (low anatomical complexity). The patient underwent successful multivessel percutaneous coronary intervention (PCI) using contemporary drug-eluting stents, including a double-kissing crush technique for a LAD–diagonal bifurcation lesion, achieving final TIMI 3 flow in all treated vessels.
This case highlights warm-up angina as a manifestation of ischemic preconditioning and emphasizes that elite endurance performance does not exclude severe atherosclerotic disease. Careful evaluation of exertional symptoms in athletes, particularly those with a significant family history of SCD, remains essential.
Learning Objectives
- To recognize warm-up angina as a manifestation of ischemic preconditioning;
- To understand that severe multivessel coronary artery disease may occur in elite athletes without traditional risk factors;
- To emphasize the importance of maintaining a high index of suspicion for coronary pathology in athletes presenting with exertional symptoms.
Keywords: Warm-Up Angina; Ischemic Threshold; Marathon Athlete; Coronary Artery Disease; Percutaneous Coronary Intervention; Atypical Chest Pain; Endurance Exercise
INTRODUCTION
Chest pain in endurance athletes represents a diagnostic challenge. Although most symptoms are non-cardiac in origin, ischemic etiologies can occur even in highly trained individuals [1]. Studies have reported that 11–13% of master endurance athletes with low traditional risk profiles demonstrate significant coronary stenoses on coronary CT angiography (CCTA) [2]. Long-term endurance exercise has been associated with increased total coronary plaque burden; however, plaques in athletes are often more calcified and potentially more stable compared with the mixed or lipid-rich plaques seen in sedentary populations [3].
This paradox may delay diagnosis, as clinicians and patients alike may underestimate the possibility of obstructive coronary artery disease in individuals with exceptional physical performance [4].
We report a case of warm-up angina in a 50-year-old elite marathon runner found to have severe multivessel coronary artery disease, highlighting an important clinical phenomenon in sports cardiology.
CASE PRESENTATION
A 50-year-old male elite marathon runner presented for cardiovascular evaluation due to exertional chest discomfort. His history was notable for sudden cardiac death in three brothers between the ages of 42 and 55 years, each reportedly preceded by severe chest pain. No autopsies were performed. The patient was counseled regarding possible familial predisposition to premature coronary artery disease, and cardiovascular screening was recommended for first-degree relatives.
He had no conventional cardiovascular risk factors. He was a lifelong non-smoker, normotensive, non-diabetic, and maintained a favorable lipid profile (LDL 77 mg/dL, Lipoprotein(a) 23 mg/dL).
He was a national marathon champion who had recently placed fourth in the Berlin International Marathon and second in the India International Marathon. His training regimen included extremely high endurance volumes.
The presenting symptom consisted of a transient burning chest discomfort occurring specifically during the initial phase of running (warm-up). Notably, the discomfort subsided spontaneously with continued exertion, allowing him to complete prolonged sessions, including a recent 157 km run during which the symptom first appeared.
Resting electrocardiography was normal. Transthoracic echocardiography demonstrated normal left ventricular size and systolic function without structural abnormalities.
Given the significant family history of SCD, further evaluation was pursued. CCTA revealed calcified plaques causing significant stenoses in the LAD, RCA, and LCx arteries, consistent with multivessel coronary artery disease (Figure 1, Video 1).
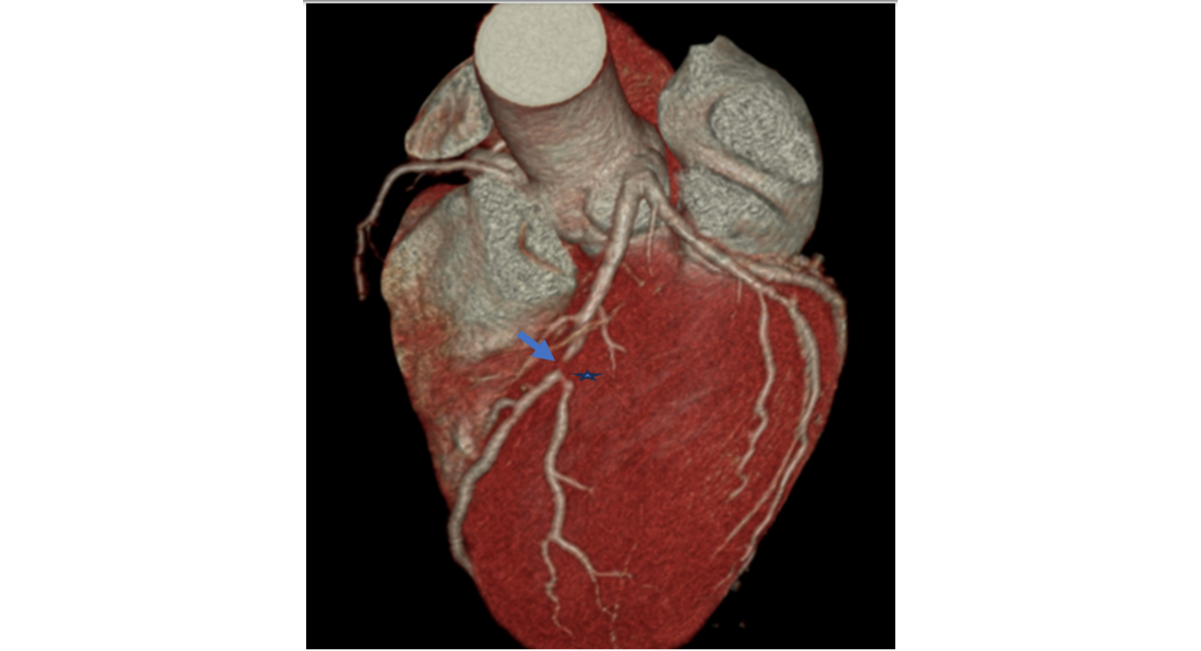
Figure 1: 3D volume-rendered CTA shows severe stenosis in the mid LAD (arrow) and second diagonal (star).
Video 1: CTA axial view demonstrating severe calcified and non- calcified atherosclerotic plaque in the mid LAD causing severe stenosis, along with severe stenosis at the ostium of the 2nd diagonal branch. Severe atherosclerotic plaque at distal RCA with severe stenosis is also noted.
https://doi.org/10.5281/zenodo.18757262
Invasive coronary angiography confirmed severe proximal LAD stenosis, significant LAD–diagonal bifurcation disease, and severe RCA stenosis. The calculated SYNTAX score was 18, indicating low anatomical complexity.
PCI was performed via right radial access. Drug-eluting stents were deployed. The LAD–diagonal bifurcation lesion, characterized by severe ostial diagonal stenosis and an unfavorable bifurcation angle, was managed using a stepwise double-kissing crush technique to ensure optimal ostial coverage. The RCA lesion was treated with predilatation, stenting, and post-dilatation using a non-compliant balloon. Final angiography demonstrated restoration of TIMI 3 flow in all treated vessels without procedural complications (Video 2).
Video 2: Coronary angiogram shows severe stenosis in the mid LAD, ostium of the 2nd diagonal, and distal RCA. The procedure addressed these critical lesions: the proximal LAD was successfully stented, the LAD–diagonal bifurcation with severe ostial disease was managed using a stepwise double-kissing crush technique, and the RCA lesion was treated with predilatation, stenting, and post-dilatation using a non-compliant balloon
https://doi.org/10.5281/zenodo.18757545
The patient was initiated on high-intensity statin therapy and dual antiplatelet therapy planned for 12 months. He was advised to resume endurance training gradually with initial avoidance of high-intensity intervals. At 6-month follow-up, he remained asymptomatic with no recurrence of exertional chest discomfort.
DISCUSSION
This case illustrates several important considerations in the evaluation of athletes with exertional symptoms.
Warm-up angina is characterized by chest discomfort at the onset of exercise that improves with continued exertion. The underlying mechanism is thought to involve ischemic preconditioning, whereby an initial brief ischemic stimulus enhances myocardial tolerance to subsequent ischemia [5]. Proposed physiological mechanisms include adenosine-mediated vasodilation, improved endothelial function, reduced myocardial oxygen demand, and recruitment of collateral circulation [6].
Although endurance exercise confers substantial cardiovascular benefit, it does not eliminate the risk of atherosclerosis. Master athletes may demonstrate increased coronary plaque burden, frequently with more calcified morphology [3]. Importantly, the absence of traditional risk factors does not preclude obstructive disease, particularly in the presence of strong familial predisposition.
The occurrence of SCD in three first-degree relatives suggests possible polygenic susceptibility to premature coronary artery disease. Although no structural cardiomyopathy was identified, familial screening and cardiovascular risk assessment are warranted in such settings.
According to AHA/ACC recommendations, pre-participation cardiovascular screening in athletes should include focused history and examination, specifically addressing exertional chest pain and family history of premature cardiovascular disease or SCD [4]. In athletes older than 35–50 years or those with significant family history, further evaluation with stress testing or coronary imaging should be considered [2,4].
This case underscores that exceptional athletic performance may mask clinically significant ischemia and that early diagnostic imaging may be appropriate when clinical suspicion is high.
CONCLUSION
Elite endurance athletes are not immune to severe multivessel coronary artery disease. Warm-up angina may represent the only clinical manifestation of significant ischemia. Careful history-taking, particularly regarding family history of sudden cardiac death, and a low threshold for advanced cardiac imaging are essential to prevent adverse outcomes. Maintaining a high index of suspicion remains critical in this unique population.
PATIENT CONSENT STATEMENT
Verbal informed consent was obtained from the patient for publication of this case report and accompanying images. All identifying information has been anonymized to protect patient confidentiality. Ethical approval was not required for this single case report in accordance with institutional policy.
COMPETING INTERESTS
The authors declare that they have no competing interests.
CONTRIBUTORSHIP
All authors contributed to the conception, drafting, revision, and final approval of the manuscript.
DISCLAIMER
The views expressed are the authors' own and not an official position of the institution.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
PATIENT INVOLVEMENT
No direct patient involvement in the manuscript preparation.
REFERENCES
- Moran B, Bryan S, Farrar T, Salud C, Visser G, Decuba R, et al. Diagnostic evaluation of nontraumatic chest pain in athletes. Curr Sports Med Rep. 2017;16(2):84-94. [Crossref] [Google Scholar] [PubMed]
- Merghani A, Maestrini V, Rosmini S, Cox AT, Dhutia H, Bastiaenan R, et al. Prevalence of subclinical coronary artery disease in masters endurance athletes with a low atherosclerotic risk profile. Circulation. 2017;136(2):126-37. [Crossref] [Google Scholar] [PubMed]
- Aengevaeren VL, Mosterd A, Braber TL, Prakken NH, Doevendans PA, Grobbee DE, et al. Relationship between lifelong exercise volume and coronary atherosclerosis in athletes. Circulation. 2017;136(2):138-48. [Crossref] [Google Scholar] [PubMed]
- Franklin BA, Thompson PD, Al-Zaiti SS, Albert CM, Hivert MF, Levine BD, et al. American Heart Association Physical Activity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Stroke Council. Exercise-related acute cardiovascular events and potential deleterious adaptations following long-term exercise training: placing the risks into perspective–an update: a scientific statement from the American Heart Association. Circulation. 2020;141(13):e705-36. [Crossref] [Google Scholar] [PubMed]
- Bogaty P, Poirier P, Boyer L, Jobin J, Dagenais GR. What induces the warm-up ischemia/angina phenomenon: exercise or myocardial ischemia? 2003;107(14):1858-63. [Crossref] [Google Scholar] [PubMed]
- Williams RP, Manou-Stathopoulou V, Redwood SR, Marber MS. ‘Warm-up Angina’: harnessing the benefits of exercise and myocardial ischaemia. Heart. 2014;100(2):106-14. [Crossref] [Google Scholar] [PubMed]
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 15 Days |
Peer Review Feedback |
| 85% | Acceptance Rate (after peer review) |
| 30-45 Days | Total article processing time |
Journal Flyer