ABSTRACT
Background
The clinical advantages of stentless compared with conventional stented bioprosthetic valves in surgical aortic valve replacement (SAVR) remain uncertain, particularly in the context of evolving lifetime valve management strategies and the increasing role of transcatheter interventions.
Objectives
To compare early clinical outcomes and hemodynamic performance between stented and stentless bioprosthetic valves used in SAVR.
Methods
A systematic review and meta-analysis were conducted in accordance with PRISMA guidelines and registered in PROSPERO. PubMed, Embase, the Cochrane Library, and Scopus were searched from database inception through September 2025. Randomized controlled trials and observational studies comparing stented and stentless bioprostheses in SAVR were included. Outcomes of interest included early clinical outcomes (in-hospital or within 30 days), together with intermediate and late hemodynamic outcomes when available. Random-effects models were used to pool effect estimates.
Results
A total of 56 studies comprising 17,260 patients were included. Early mortality, stroke, myocardial infarction, endocarditis, reoperation, and hospital length of stay were comparable between the two valve types. Stentless valves were associated with improved hemodynamic performance, demonstrated by larger effective orifice areas (mean difference [MD] 0.38 cm², 95% CI 0.28–0.48) and lower mean transvalvular gradients (MD −0.68 mmHg, 95% CI −1.05 to −0.31). Left ventricular mass regression was similar between groups. Moderate to high heterogeneity was observed across hemodynamic outcomes.
Conclusion
Stentless bioprosthetic valves demonstrate superior hemodynamic performance compared with stented valves but do not appear to improve early clinical outcomes. Given the predominance of observational evidence and the growing importance of lifetime valve management strategies, including valve-in-valve feasibility, prosthesis selection should be individualized.
Keywords: Aortic Valve Replacement; Stented Valve; Stentless Valve; Hemodynamics; Mortality; Systematic Review; Meta-Analysis
INTRODUCTION
Aortic valve disease predominantly aortic stenosis and aortic regurgitation represent the most prevalent acquired valvular pathology among adults. Both conditions share degenerative and calcific etiologies that progressively impair normal leaflet motion and valve closure, leading to chronic left ventricular (LV) pressure and/or volume overload. These hemodynamic stresses trigger concentric or eccentric LV hypertrophy and remodeling; processes independently associated with an increased risk of adverse cardiovascular outcomes and mortality [1]. Surgical aortic valve replacement (AVR) remains the definitive treatment for severe disease, as medical therapy alone confers a poor prognosis, with symptomatic severe aortic stenosis associated with markedly increased mortality if left untreated [2]. Despite procedural success, long-term survival remains suboptimal, partly due to incomplete regression of LV hypertrophy and the hemodynamic limitations inherent to certain prosthetic valve designs [2,3].
Bioprosthetic valves derived from porcine or bovine tissue have gained preference over mechanical valves in elderly patients because of their lower thrombogenic potential and the avoidance of lifelong anticoagulation. However, their durability remains limited by structural tissue degeneration (STD), often influenced by patient age, fixation methods, and mechanical stress [4]. The development of stentless bioprosthetic valves aimed to overcome the geometric and flow restrictions associated with stented designs by increasing the effective orifice area (EOA) and reducing transvalvular gradients [1,4]. By eliminating the stent and sewing ring, stentless valves theoretically offer more physiological flow dynamics and enhanced regression of LV hypertrophy compared with their stented counterparts [5,6].
Numerous clinical studies have evaluated the hemodynamic performance and clinical outcomes associated with stentless versus stented bioprosthetic valves. While smaller cohort studies and mid-term analyses have demonstrated lower transvalvular gradients, larger EOAs, and more complete LV mass regression with stentless valves, results from randomized controlled trials (RCTs) have been inconsistent [1,2,5]. Variability in surgical technique, valve model, patient characteristics, and follow-up duration has contributed to these conflicting findings, leaving uncertainty regarding the true clinical superiority of one design over the other. Furthermore, although improved hemodynamics may theoretically translate into more pronounced LV mass regression a surrogate marker of better survival definitive evidence linking valve design to long-term survival or reduced reoperation rates remains limited [6].
Left ventricular hypertrophy itself is a well-established independent predictor of cardiovascular morbidity and mortality in both the general population and in patients with valvular heart disease [3]. Echocardiographic studies, notably from the Framingham cohort, have demonstrated that increased LV mass strongly correlates with higher risks of coronary heart disease and all-cause mortality, even after adjustment for conventional risk factors [3]. Therefore, the extent of LV mass regression following AVR serves as a key determinant of postoperative prognosis and an essential endpoint in evaluating prosthetic valve performance.
Given the persistent uncertainty and the clinical importance of optimizing postoperative outcomes, an updated synthesis of the available evidence is warranted. The previous meta-analysis by Cheng et al. was published in 2009 and included substantially fewer studies conducted before the widespread adoption of contemporary bioprostheses and evolving lifetime valve management strategies. Since then, additional randomized and observational studies have become available. Therefore, this systematic review and meta-analysis aim to compare stented versus stentless bioprosthetic aortic valves in adult patients undergoing surgical AVR. The analysis focuses on all-cause mortality and survival as primary outcomes, and hemodynamic performance parameters including mean gradient, effective orifice area, LV mass regression, paravalvular leak, stroke, and reoperation rates as secondary outcomes. By synthesizing contemporary evidence from randomized and observational studies, this review seeks to clarify whether the theoretical advantages of stentless bioprostheses translate into meaningful clinical benefit in modern cardiac practice.
MATERIALS AND METHODS
Study Design and Registration
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD420251142083) to ensure methodological transparency and adherence to predefined study methods.
Search Strategy
A comprehensive electronic literature search was performed from database inception through September 2025 using PubMed, Cochrane Library, and Scopus. The search strategy included combinations of the following keywords and Medical Subject Headings (MeSH) terms: (“stented aortic valve” OR “stented bioprosthetic valve”) AND (“stentless aortic valve” OR “stentless bioprosthetic valve”) AND (“aortic valve replacement” OR “AVR”). The search was limited to studies involving human subjects and published in English. In addition, the reference lists of all included articles and relevant review papers were manually screened to identify additional eligible studies. The complete electronic search strategy is provided in the Supplementary Materials (supplementary table 1).
Eligibility Criteria
Studies were considered eligible if they included adult patients aged 18 years or older undergoing surgical aortic valve replacement and provided a direct comparison between stented and stentless bioprosthetic valves. Both randomized controlled trials and observational cohort studies were included. Studies were excluded if they were conference abstracts, editorials, letters, case reports, review articles, animal studies, non-English publications, or did not report comparative data between the two valve types. Only English-language studies were included to ensure accurate data extraction and risk-of-bias assessment. This restriction may have introduced language bias.
Study Selection
Two independent reviewers screened titles and abstracts for potential eligibility. Full-text articles were subsequently assessed for inclusion according to the predefined criteria. Disagreements between reviewers were resolved through discussion and consensus. The study selection process followed PRISMA recommendations, and a flow diagram summarizing the screening and inclusion process is presented in Figure 1.
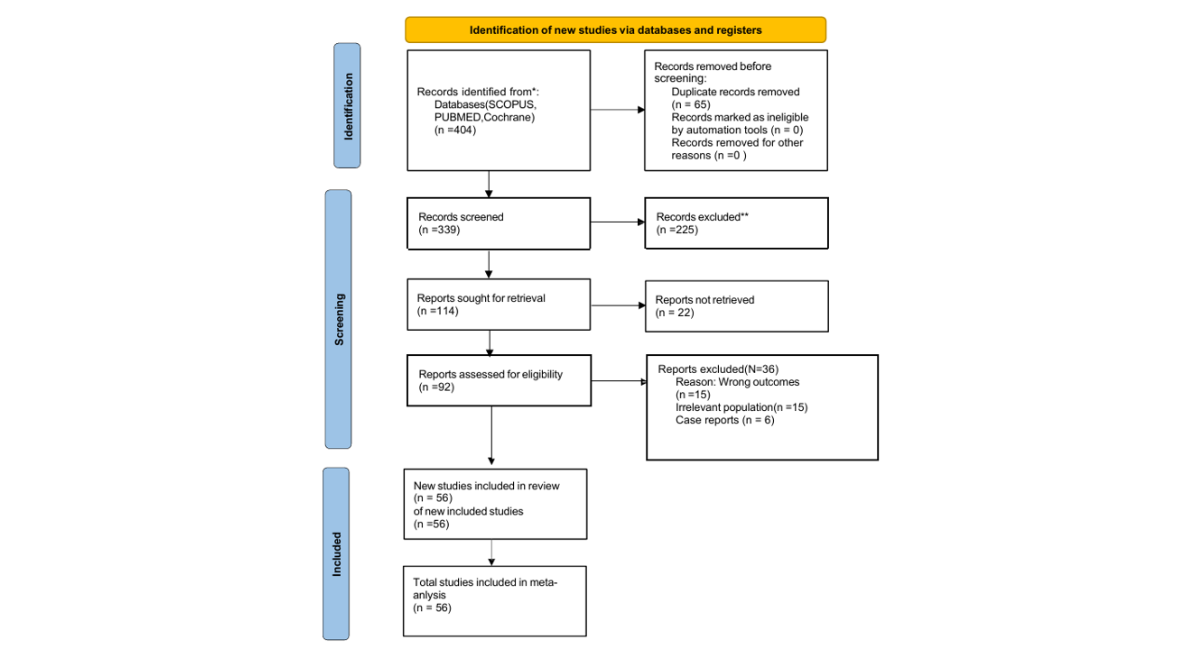
Figure 1: Prisma Flowchart
Data Extraction
Data extraction was performed independently by two reviewers using a standardized data collection form. Extracted information included study characteristics (author, year of publication, country, study design, and study period), patient demographics (sample size, group-specific sample sizes, mean age, sex distribution, comorbidities, baseline left ventricular function, and aortic annulus size when available), and operative details such as valve type and material, valve size, implantation technique when reported, cross-clamp time, and cardiopulmonary bypass time. Information regarding clinical outcomes, hemodynamic parameters, duration of follow-up, and reported study limitations was also collected.
Outcome Definitions
Outcomes were categorized according to the timing of assessment to improve clinical interpretability. Early outcomes were defined as events occurring during hospitalization or within 30 days after surgery. Intermediate outcomes were defined as assessments performed between 6 and 12 months postoperatively, whereas late outcomes were defined as those reported beyond one year of follow-up. Early clinical outcomes included mortality, stroke, myocardial infarction, endocarditis, reoperation, paravalvular leak, and length of hospital stay. Hemodynamic outcomes included effective orifice area, mean transvalvular pressure gradient, and left ventricular mass or left ventricular mass index regression.
Risk of Bias Assessment
Risk of bias was independently assessed by two reviewers. Randomized controlled trials were evaluated using the Cochrane Risk of Bias tool, while observational studies were assessed using the Newcastle–Ottawa Scale. Any disagreements were resolved through consensus. Detailed risk-of-bias assessments for all included studies are provided in the Supplementary Materials.
Statistical Analysis
Statistical analyses were performed using Review Manager (RevMan version 5.4, Cochrane Collaboration). Dichotomous outcomes were pooled using risk ratios with 95% confidence intervals, while continuous outcomes were analyzed using mean differences with 95% confidence intervals. A random-effects model based on the DerSimonian Laird method was applied to account for expected clinical and methodological heterogeneity among studies. Statistical heterogeneity was assessed using the chi-square test, τ², and the I² statistic, with values of 50% or greater considered indicative of substantial heterogeneity. A two-sided P value of less than 0.05 was considered statistically significant.
Sensitivity and Subgroup Analyses
Sensitivity analyses were performed by comparing the results obtained using fixed-effects and random-effects models and by conducting leave-one-out analyses to evaluate the influence of individual studies on pooled estimates. Subgroup analyses were conducted according to the timing of outcome measurement (early, intermediate, and late follow-up). Prespecified subgroup analyses according to study design (RCTs versus observational studies) were performed whenever sufficient data were available and are emphasized throughout the Results.
Artificial Intelligence Disclosure
ChatGPT (OpenAI) was used solely for language editing and grammatical refinement. No artificial intelligence tools were used for study selection, data extraction, statistical analysis, or interpretation of the findings.
RESULTS
The database search yielded 404 records. After removal of 65 duplicates, 339 records underwent title and abstract screening. Ninety-two full-text articles were assessed for eligibility, of which 56 studies met the inclusion criteria and were included in the qualitative and quantitative synthesis (Figure 1).
Our study focuses on comparison between stented and stentless aortic valve procedures in different aspects. Our main endpoints are early all causes- mortality rates, stroke, MI, endocarditis rates and hemodynamic responses at different times ranging from early or pre-discharge to more than one year.
So, our study included 17260 patients who underwent aortic valve procedures for different indications, 12651 patients have stented valves and the other 4609 patients had stentless aortic valve [2,4,5, 7, 8-10, 17-63]. For patients' characteristics. Supplementary Table.1
Early All Causes Mortality Rates
During our systematic review we noticed that all or nearly all studies focused on early mortality and its causes. Not all studies focused on long-term mortality rates; however, they mentioned survival rates without enough data to be included in our meta-analysis. So, we focused on early mortality rates which included hospital mortalities and 30 days mortalities, whatever the cause is. Our meta-analysis included 12161 patients with stented valves and other 4065 with stentless ones. There was no statistical difference between the 2 groups [RR=1.2, 95%CI [0.92:1.57], P-value=0.1753] (Fig 2).
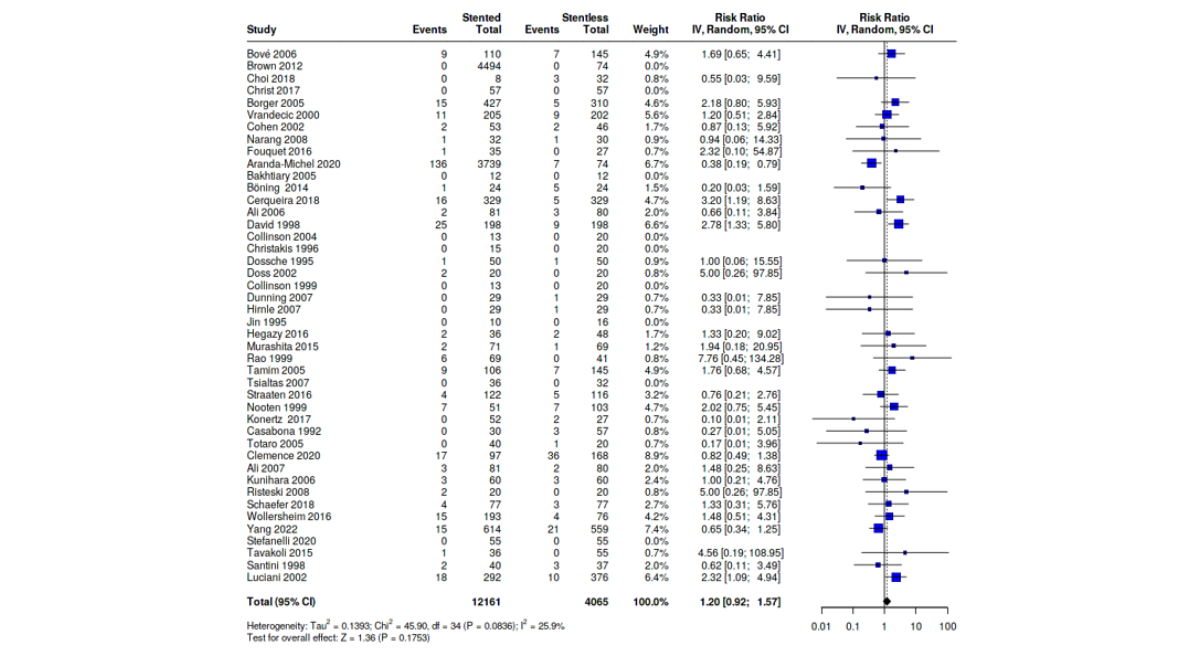
Figure 2: Forest Plot Shows Analysis of Mortality Rates Between Stented and Stentless Group
Stroke, MI and Endocarditis Rates
Stroke, MI and bacterial endocarditis are major complications that follow cardiac surgeries especially valve procedures. So, it was important to put their rates as a primary endpoint for our meta-analysis. Stroke rate meta-analysis included 11411 patients with stented valves and 3247 with stentless ones, however, it showed no statistically significant results [RR=1.03, 95%CI [0.74:1.45], P-value=0.8501] (Fig 3). MI rates analysis included 1421 patients with stented valves and 1531 with stentless ones, it also showed no statistically significant results [RR=1.06, 95%CI [0.52:2.14], P-value= 0.8819] (Fig 4). Bacterial endocarditis rate analysis also showed no statistically significant results with 6651 patients with stented valves and 2440 with stentless ones [RR=1.18. 95%CI [0.69:2.02], P-value= 0.5393 (Fig 5).
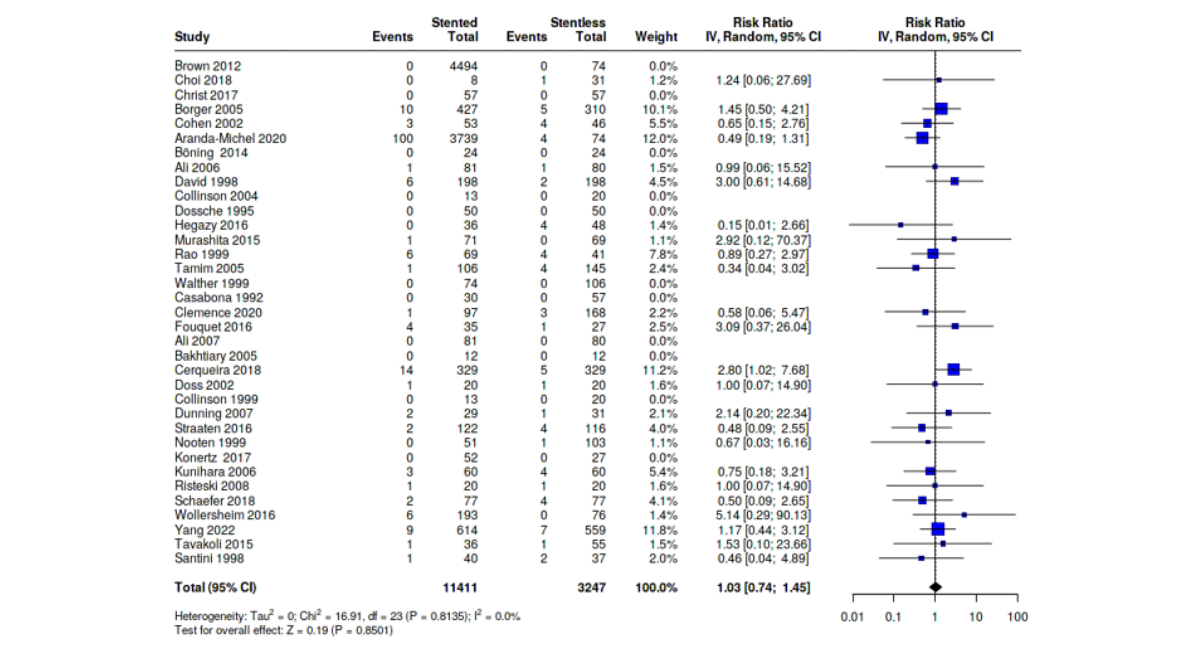
Figure 3: Forest Plot Shows Analysis of Stroke Rates Between Stented and Stentless Group
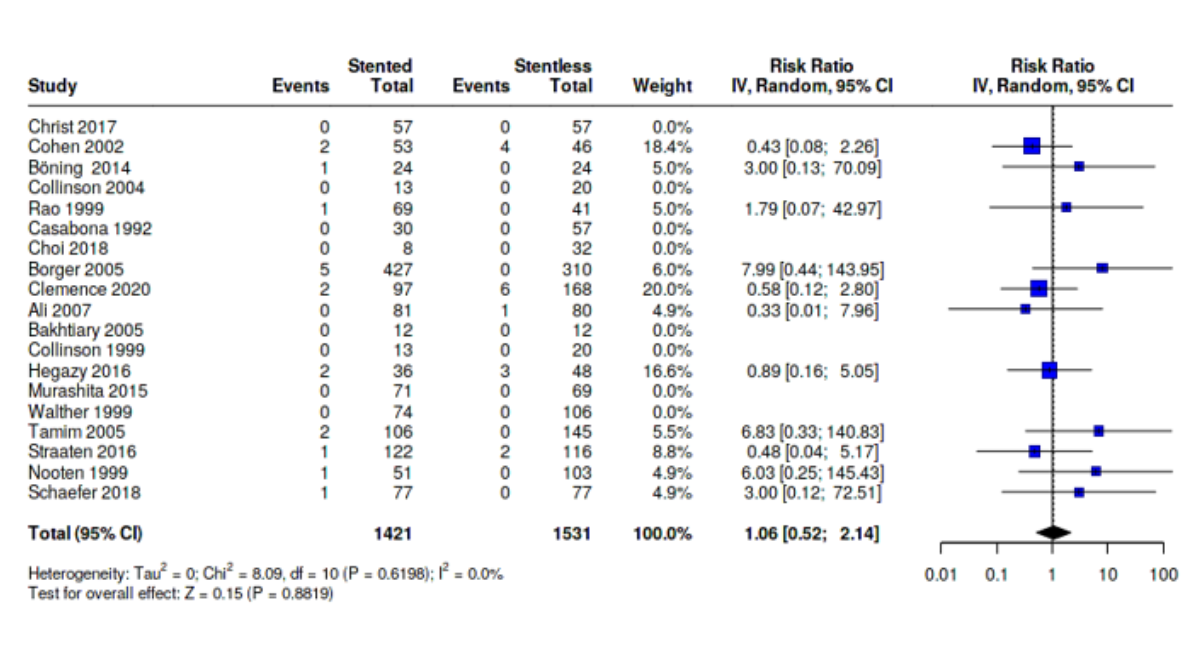
Figure 4: Forest Plot Shows Analysis of MI Rates Between Stented and Stentless Group
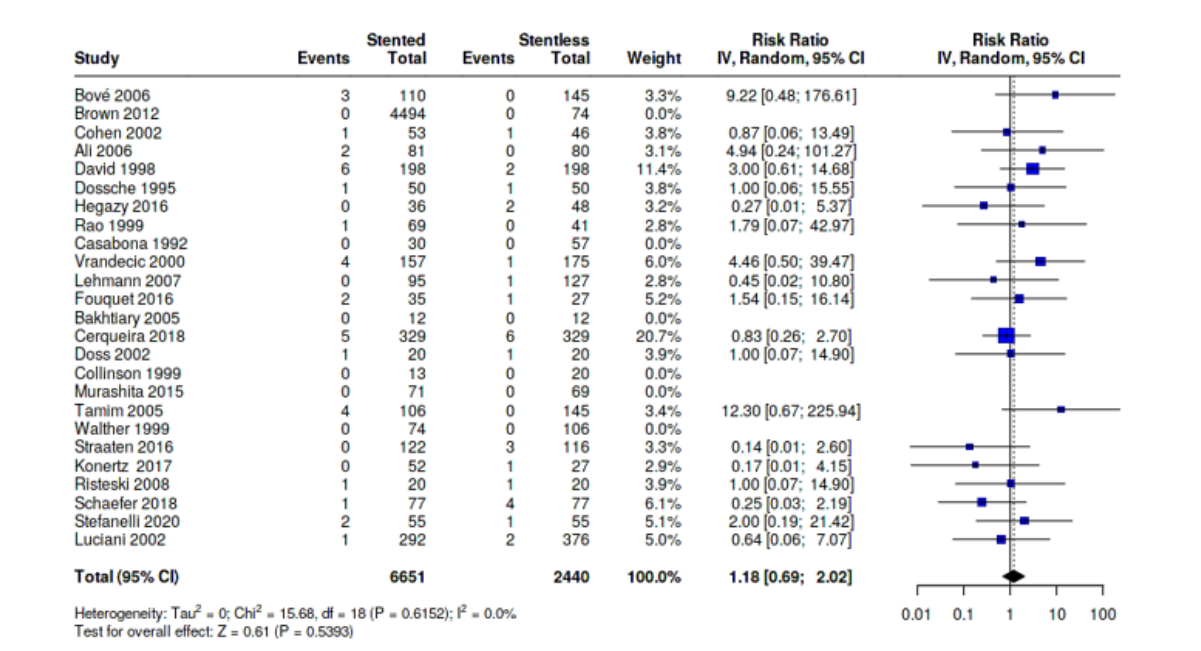
Figure 5: Forest Plot Shows Analysis of Bacterial Endocarditis Rates Between Stented and Stentless Group.
Reoperation Rates
Among studies reporting reoperations, indications frequently included surgical re-exploration for bleeding rather than prosthesis-related structural failure; however, definitions varied considerably across studies. We included 3005 in stented valve group and 3190 in stentless one. It also showed no statistically significant results [RR=0.93, 95%CI [0.69:1.25], P-value= 0.6205 (Fig 6).
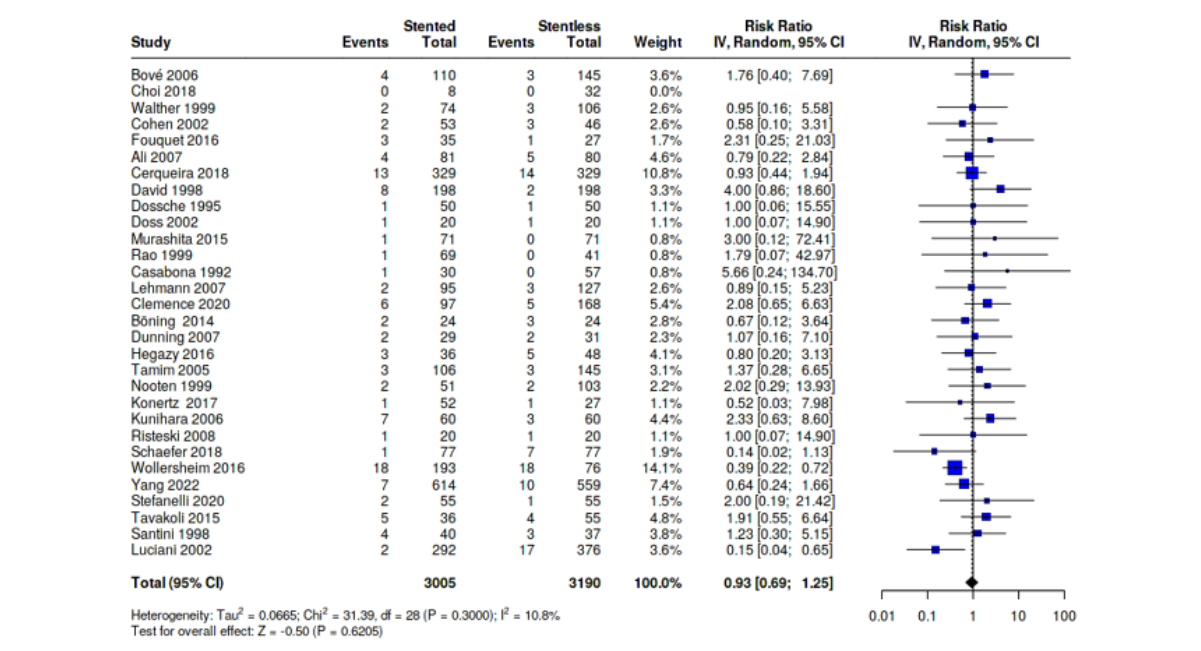
Figure 6: Forest Plot Shows Analysis of Re-Operation Rates Between Stented and Stentless Group.
Hospital Stays
By default, hospital stay is a key factor that should be included in any study as the UpToDate approaches in medicine are to shorten hospital stay and promote early recovery and rehabilitation. The analysis included 5513 with stented valves and 1664 with stentless ones, however, it showed no statistical difference between the 2 groups [MD=0.02, 95%CI [-0.23:0.27], P-value= 0.8836] (Fig 7). We conducted Leave-One-Out sensitivity analysis by removing Aranda-Michel from meta-analysis and heterogeneity dropped to 80.7% [7].
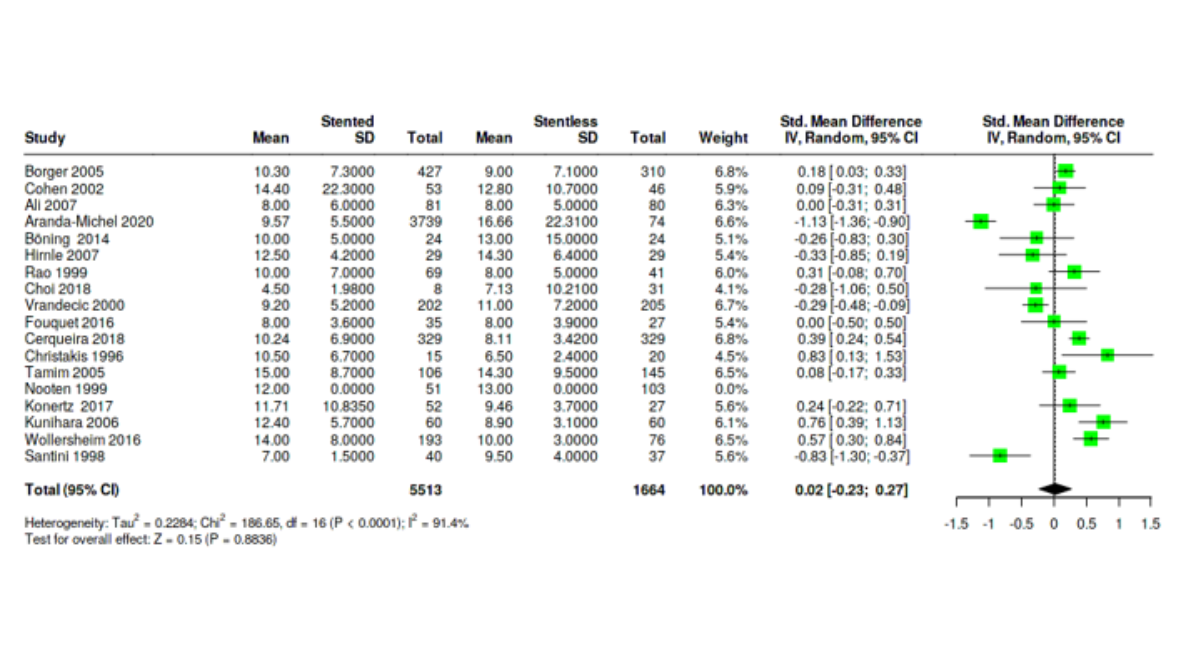
Figure 7: Forest Plot Shows Analysis of Hospital Stay Times Between Stented and Stentless Group.
Hemodynamics of The Valves
This is our major primary endpoint of this study. It includes 3 endpoints:
Effective Orifice Area (EOA) Cm2
EOA is measured on different occasions and not at a single point of time, so we sub-grouped studies that measure it according to time of measurement into 2 subgroups: early (at discharge) and late (at 12 months postoperatively). Analysis showed no statistically significant difference between stented and stentless valves in early period [MD= -0.16, 95%CI [-0.41:0.9], P-value= 0.2030] (fig. S1). Subgroup analysis showed: study design; RCT (RR=-0.51, 95%CI [-1.69:0.67]), and observational (RR=-0.24, 95%CI [-0.55:0.08]) and time; before 2010(RR=-0.07, 95%CI [-0.31:0.17]), and after 2010 (RR=-0.85, 95%CI [-1.88:0.18].
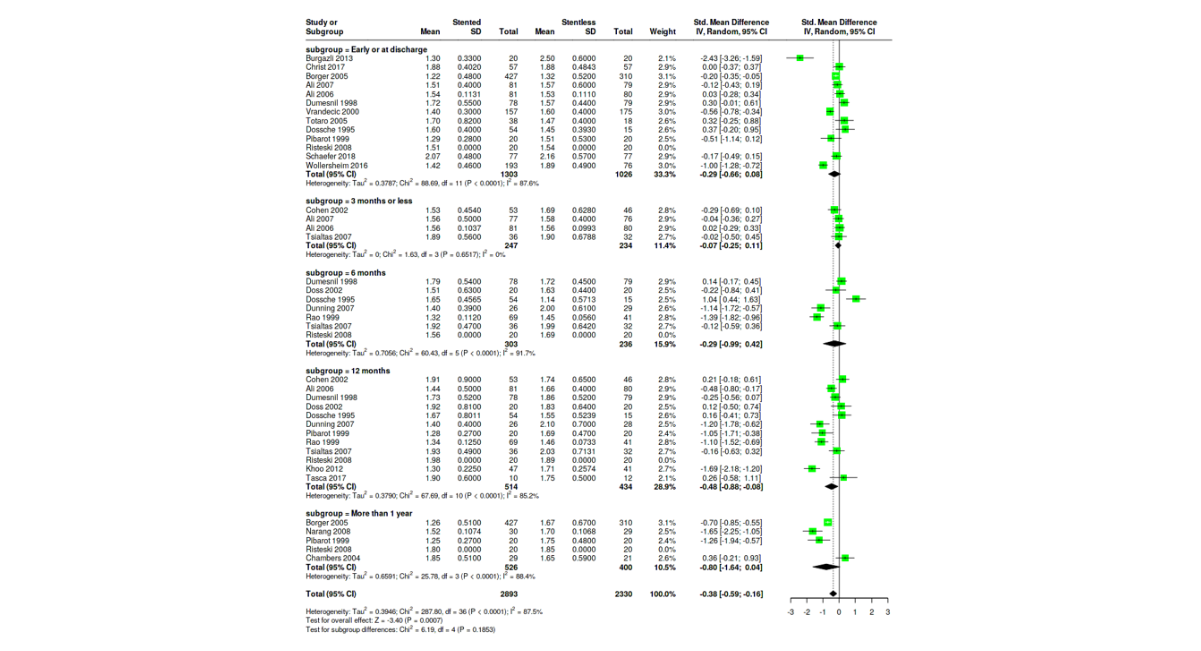
Figure S1: Forest Plot Shows Analysis of Effective Surface Area (EOA) Between Stented and Stentless Group
But in late period there was statistically significant difference in favor of stentless valves [MD= -0.48, 95%CI [-0.88: -0.08], P-value=0.0178]. Subgroup analysis showed: study design; RCT (RR=-0.24, 95%CI [-0.77:0.3]), and observational (RR=-0.68, 95%CI [-1.24:-0.11]) and time; before 2010 (RR=-0.41, 95%CI [-0.77:-0.05]), and after 2010 (RR=-0.74, 95%CI [-2.66:1.17])
Mean Pressure Gradient Mmhg
Mean transvalvular pressure gradient is an important factor in hemodynamics. We sub grouped studies according to time of measurements also into 2 subgroups: early (at discharge) and late (at 12 months postoperatively). Analysis showed statistically significant difference in favor of stentless valves in early period [MD= 0.57, 95%CI [0.12:1.02], P-value= 0.0123] (fig. S2). Subgroup analysis showed: study design; RCT (RR=0.02, 95%CI [-0.92:0.97]), and observational (RR=0.72, 95%CI [0.22:1.21]) and time; before 2010 (RR=0.82, 95%CI [0.29:1.35]), and after 2010 (RR=0.11, 95%CI [-0.66:0.87]) (fig. S2).
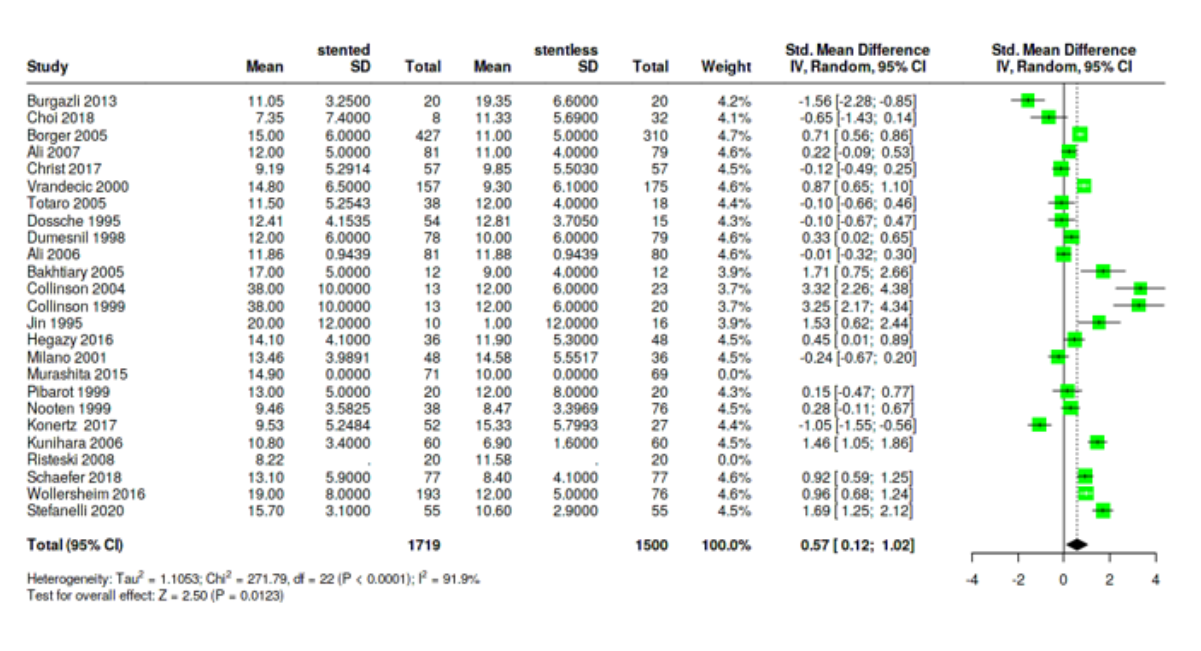
Figure S2: Forest Plot Shows Analysis of Transvalvular Mean Gradient Between Stented and Stentless Group in Early Period
Analysis also showed statistically significant difference in favor of stentless valves in late period [MD= 0.86, 95%CI [0.26:1.47], P-value=0.0052] (fig. S2). Subgroup analysis showed: study design; RCT (RR=0.18, 95%CI [-0.5:0.87]), and observational (RR=1.18, 95%CI [0.41:1.96]) and time; before 2010 (RR=0.54, 95%CI [0.11:0.96]), and after 2010 (RR=1.79, 95%CI [-0.18:3.75]) (fig.S3).
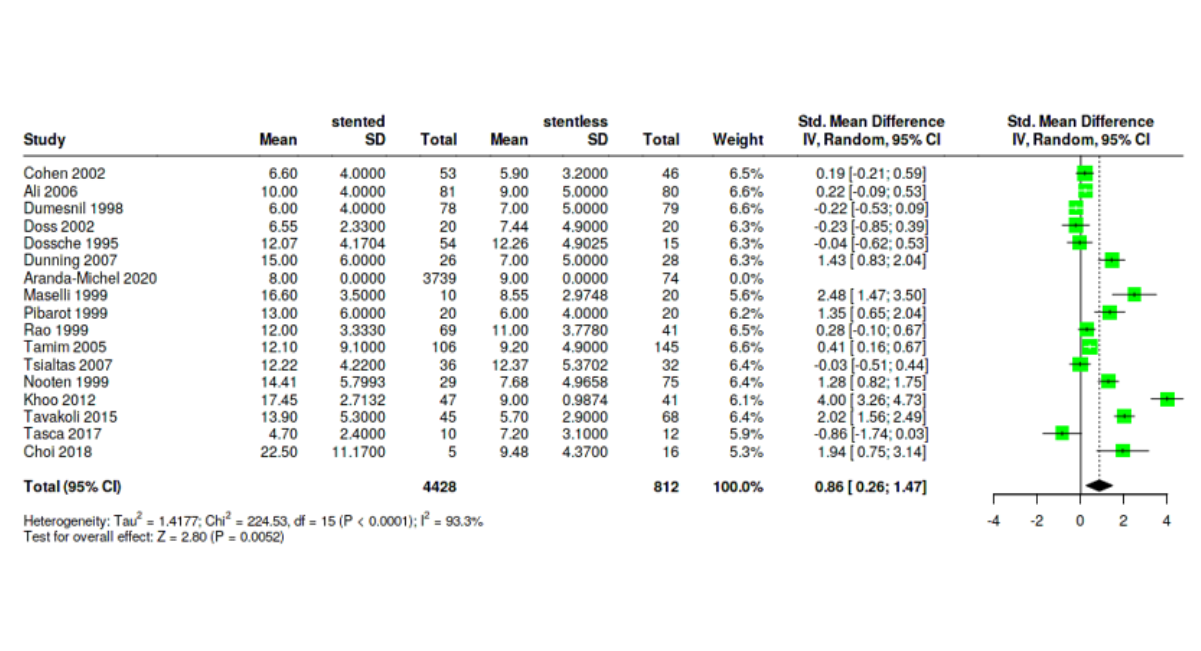
Figure S3: Forest Plot Shows Analysis of Transvalvular Mean Gradient Between Stented and Stentless Group in Late Period
Left Ventricle Regression Mass (LVRM)
We also subgrouped this outcome into early (at discharge) and late (at 12 months postoperatively) periods according to time of measurement. In early period, analysis showed no statistically significant difference between the 2 groups [MD= 0.07, 95%CI [-0.07:0.2], P-value=0.3281] (fig. S4). Subgroup analysis showed: study design; RCT (RR=0.01, 95%CI [-0.27:0.3]), and observational (RR=0.08, 95%CI [-0.1:0.25]) and time; before 2010 (RR=0.03, 95%CI [-0.15:0.22]), and after 2010; only one study Cerqueira et.al 2018 (RR=0.1, 95%CI [-0.05:0.26]).
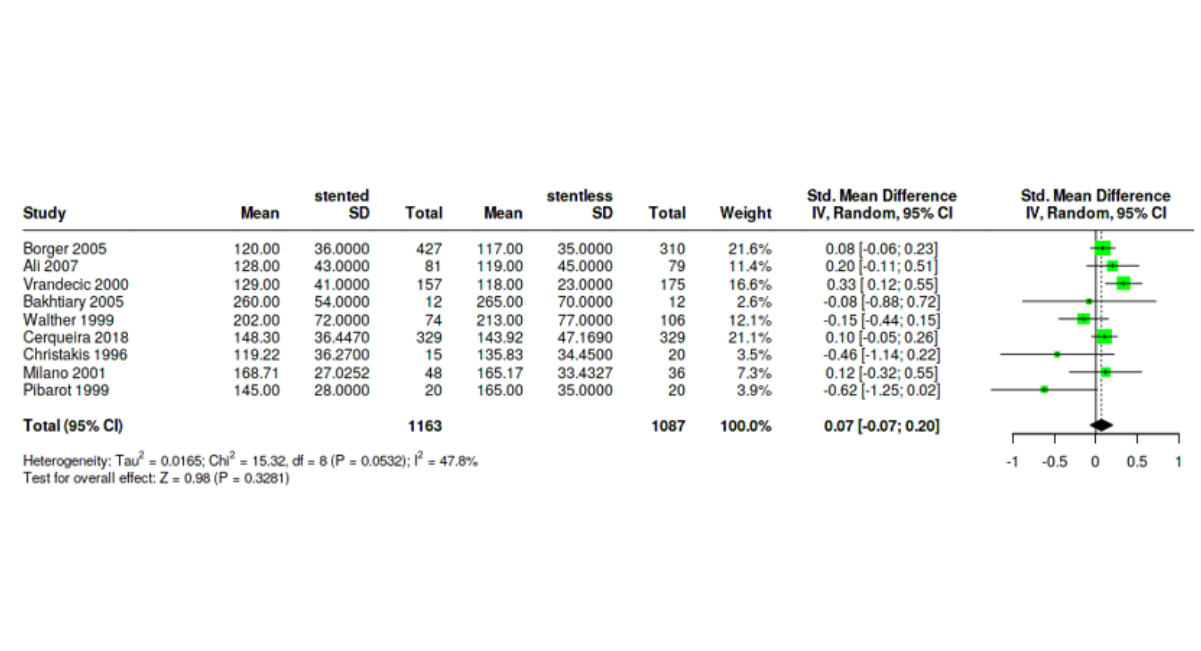
Figure S4: Forest Plot Shows Analysis of Lt Ventricle Mass (LVM) Between Stented and Stentless Group in Early Period
In late period, there was also no significant difference between the 2 groups [MD= 0.23, 95%CI [-0.14:0.6], P-value= 0.2192] (fig. S5). Subgroup analysis showed: study design; RCT (RR=0.04, 95%CI [-0.21:0.28]), and observational (RR=0.34, 95%CI [-0.37:1.05]) and time; before 2010 (RR=0.16, 95%CI [-0.23:0.54]), and after 2010; only one study Tavakoli 2015 (RR=0.86, 95%CI [0.47:1.26]).
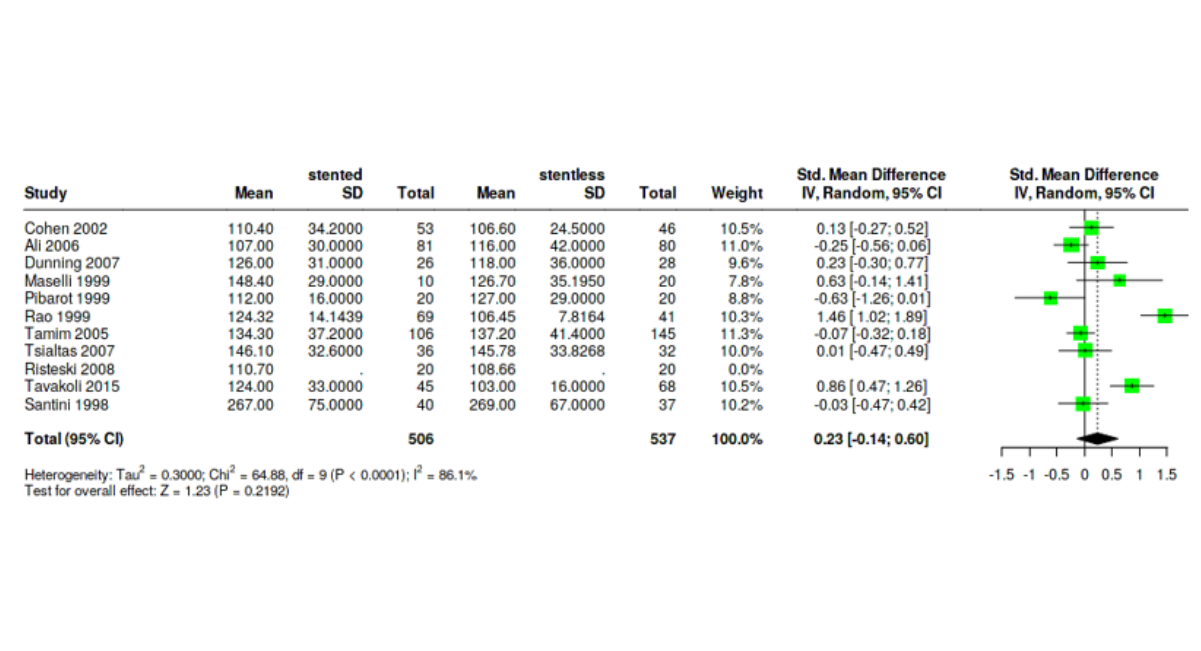
Figure S5: Forest Plot Shows Analysis of Lt Ventricle Mass (LVM) Between Stented and Stentless Group in Late Period
Paravalvular Leak Rate
Not all studies mentioned their paravalvular leak rate (PVL), but data was enough to conduct our meta-analysis to give a clue about one of the most important results in any valve procedure. We included mild, moderate and severe regurgitation in our analysis but not trivial ones and it showed that there is no statistical significance between the 2 groups [RR=1.33, 95%CI [0.58:3.04], P-value= 0.5008] (fig. S5). Subgroup analysis showed: study design; RCT (RR=1.68, 95%CI [0.32:8.82]), and observational (RR=1.16, 95%CI [0.39:3.44]) and time; before 2010 (RR=1.41, 95%CI [0.4:4.99]), and after 2010 (RR=1.1, 95%CI [0.26:4.61]) (fig. S6).
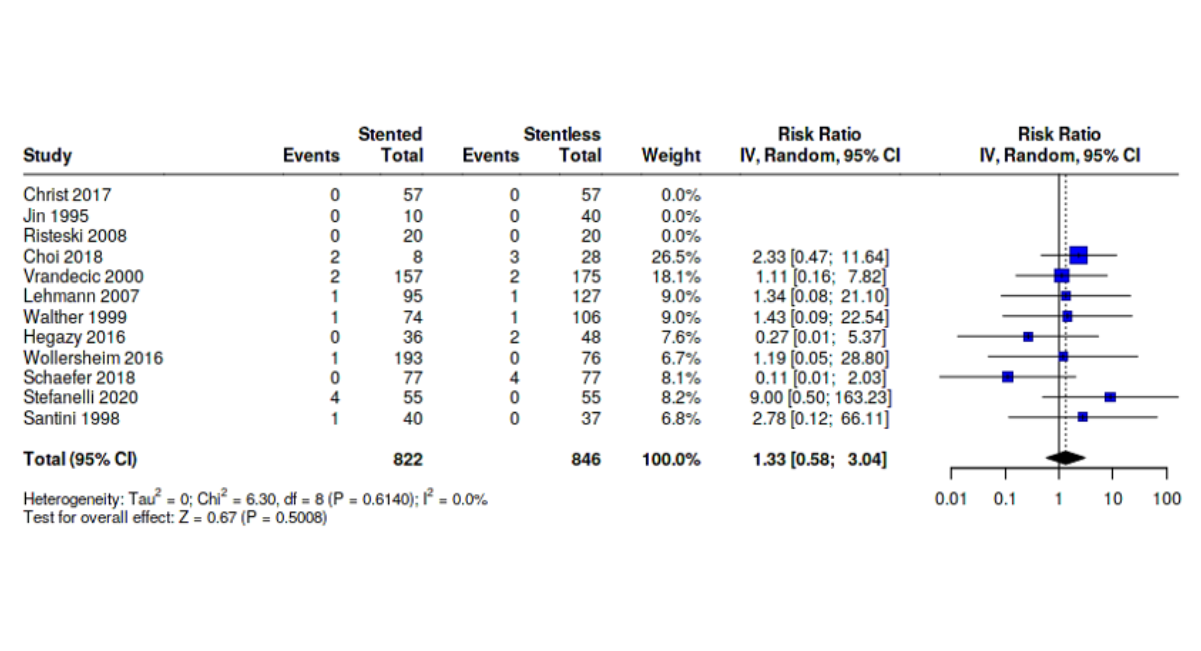
Figure S6: Forest Plot Shows Analysis of Paravalvular Leak Rates Between Stented and Stentless Group
Heterogeneity
High heterogeneity was observed in some plots of some outcomes with I2 ranging from 67.9% to 90.5%. Such substantial heterogeneity persisted even after using random effect model, performing subgrouping during analysis and performing Leave-One-Out sensitivity analysis indicating that no single study disproportionately influenced the overall results. The observed heterogeneity likely reflects clinical and methodological variability among the included studies such as patients' characteristics, surgical indications and techniques, prothesis types, variation of follow-up times. Using same study multiple times during analysis in different subgroups also contributed greatly to the overall heterogeneity. Despite the high heterogeneity, the direction of effect remained generally consistent supporting the overall findings.
Publication Bias
We assessed publication bias of each outcome of those who are mentioned previously in results section by funnel plots and eager tests. We found out that: MI rates, re-operation rates show possible publication bias supported by asymmetry of the plot and eager test values of: intercept: 2.03, 95% CI:0.64 - 3.41, t: 2.868, p-value: 0.019 and intercept: 0.91, 95% CI:0.06 - 1.76, t: 2.09, p-value: 0.046, respectively (Fig S7-18).
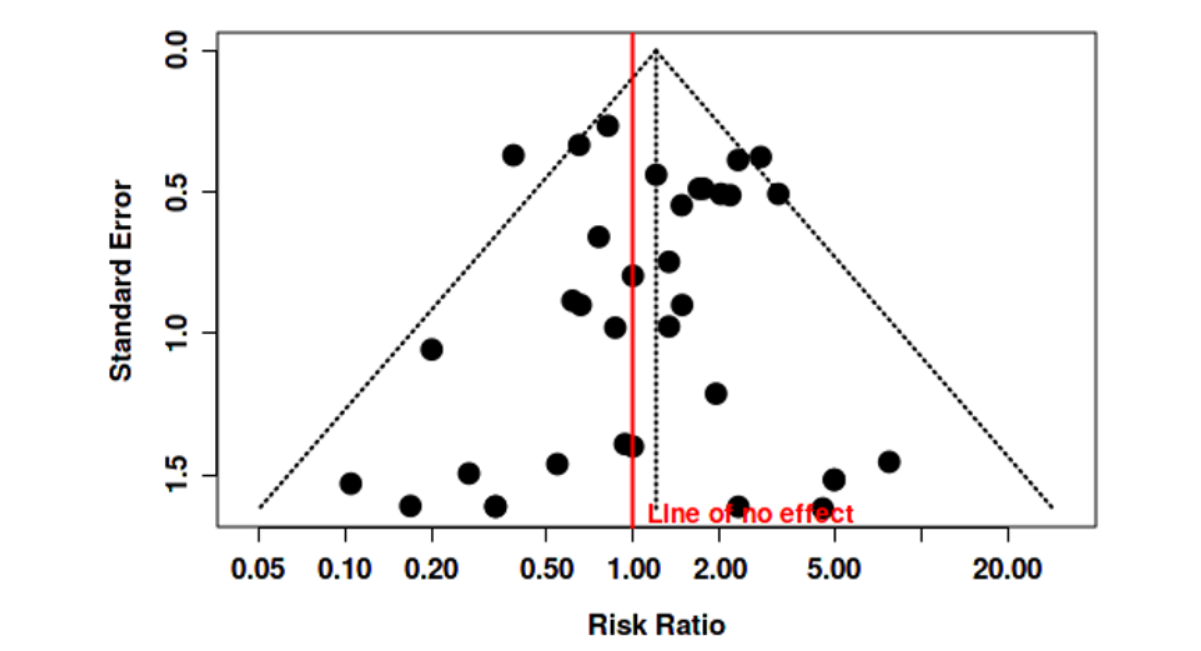
Figure S7: Funnel Plot Shows No Publication Bias of Mortality Rates Between Stented and Stentless Group.
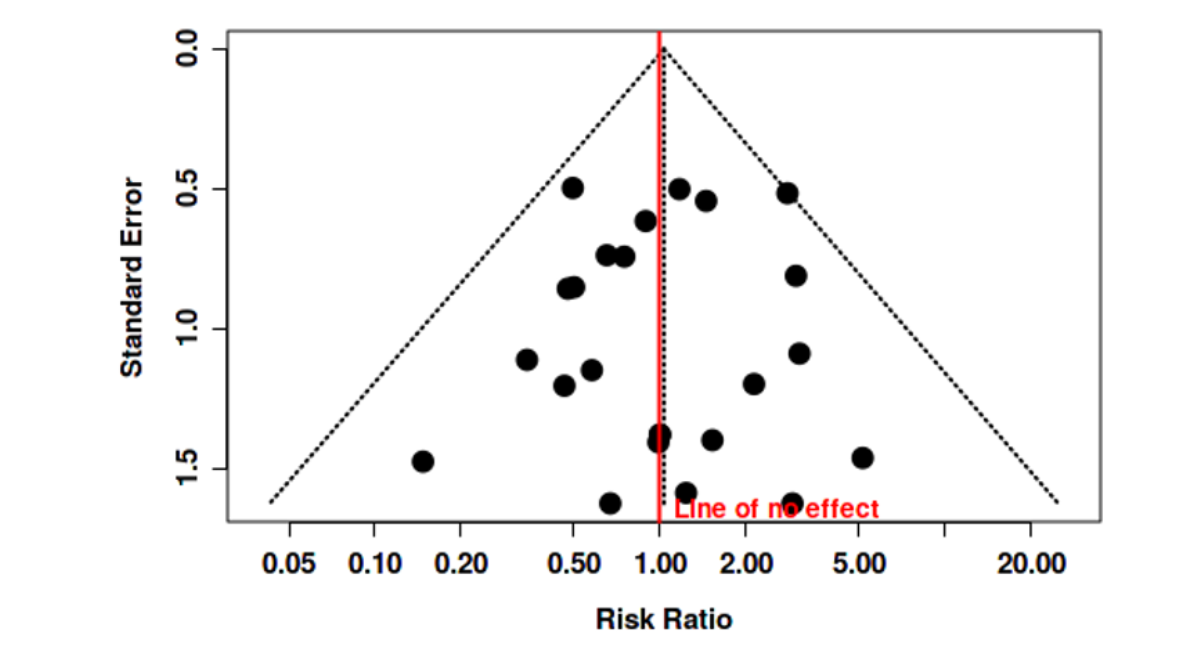
Figure S8: Funnel Plot Shows No Publication Bias of Stroke Rates Between Stented and Stentless Group.
Figure S9: Funnel Plot Shows Possible Publication Bias of MI Rates Between Stented and Stentless Group Supported by Asymmetry of The Plot and Eager Test Values Of: Intercept: 2.03, 95% CI:0.64 - 3.41, T: 2.868, P-Value: 0.019
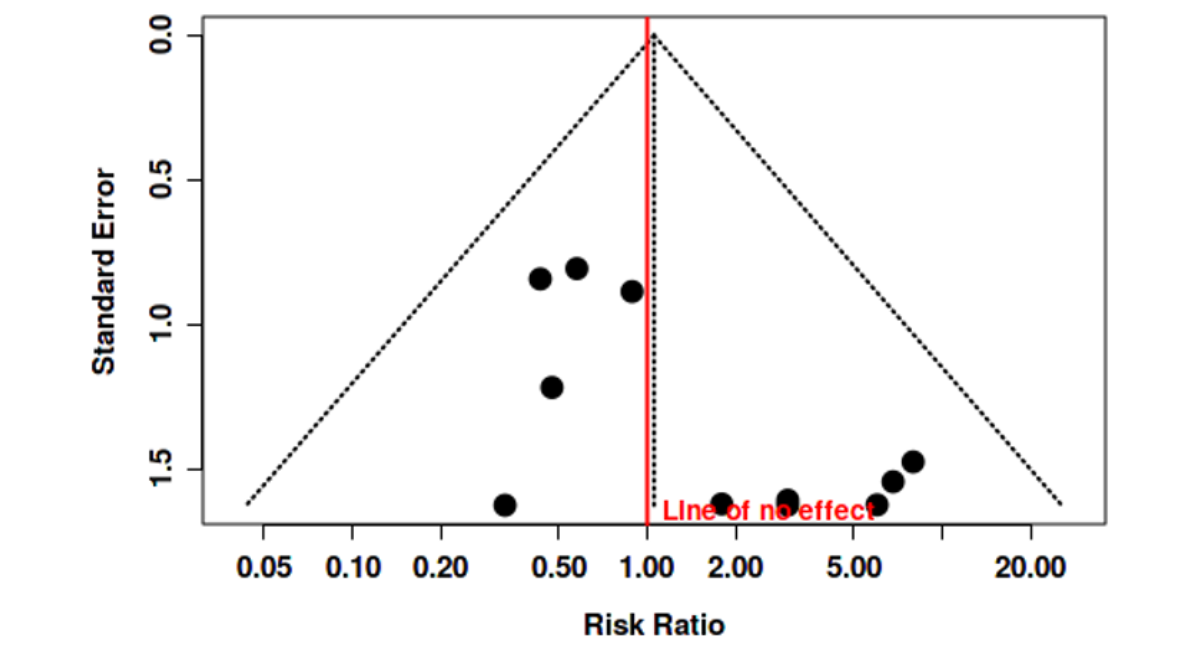
Figure S10: Funnel Plot Shows No Paublication Bias Of Bacterial Endocarditis Rates Between Stented And Stentless Group
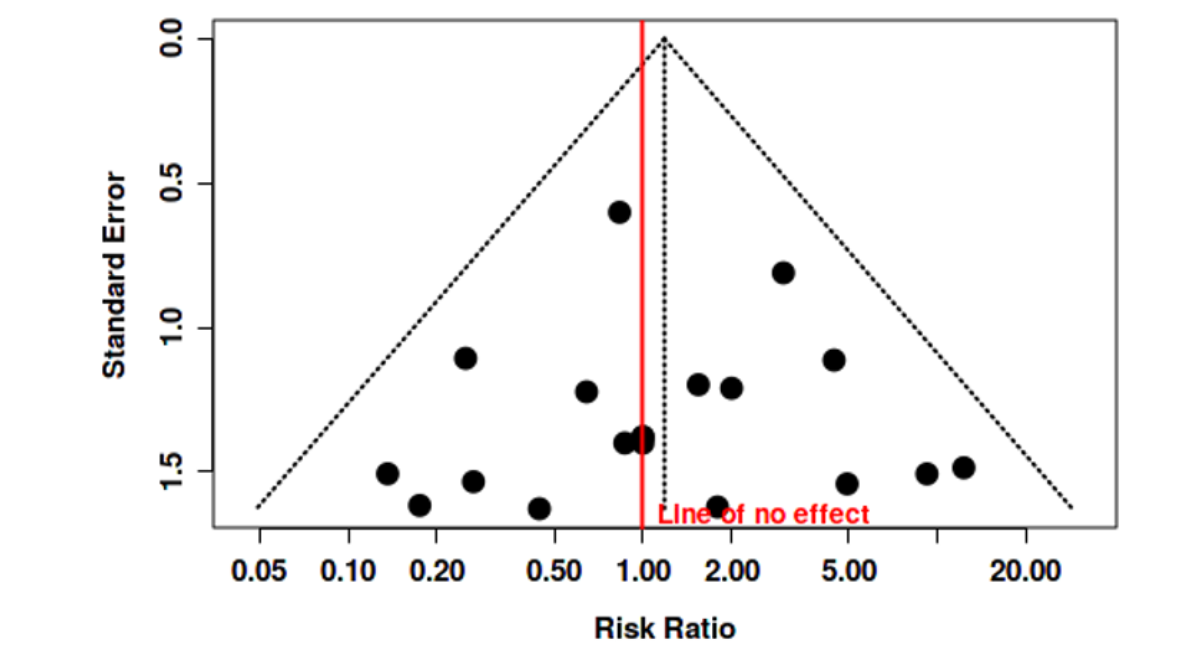
Figure S11: Funnel Plot Shows No Publication Bias of Hospital Stay Times Between Stented and Stentless Group
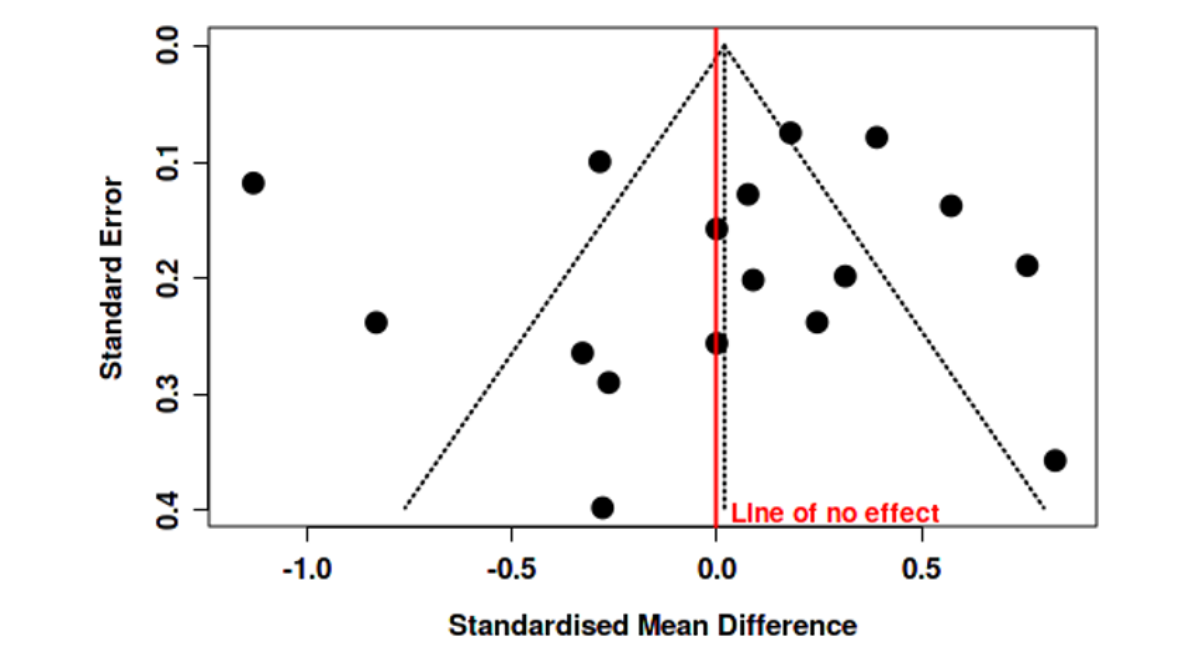
Figure S12: Funnel Plot Shows Possible Publication Bias of Re-Operation Rates Between Stented and Stentless Group Supported by Asymmetry of the Plot and Eager Test Values Of: Intercept: 0.91, 95% CI:0.06 - 1.76, T: 2.09, P-Value: 0.046
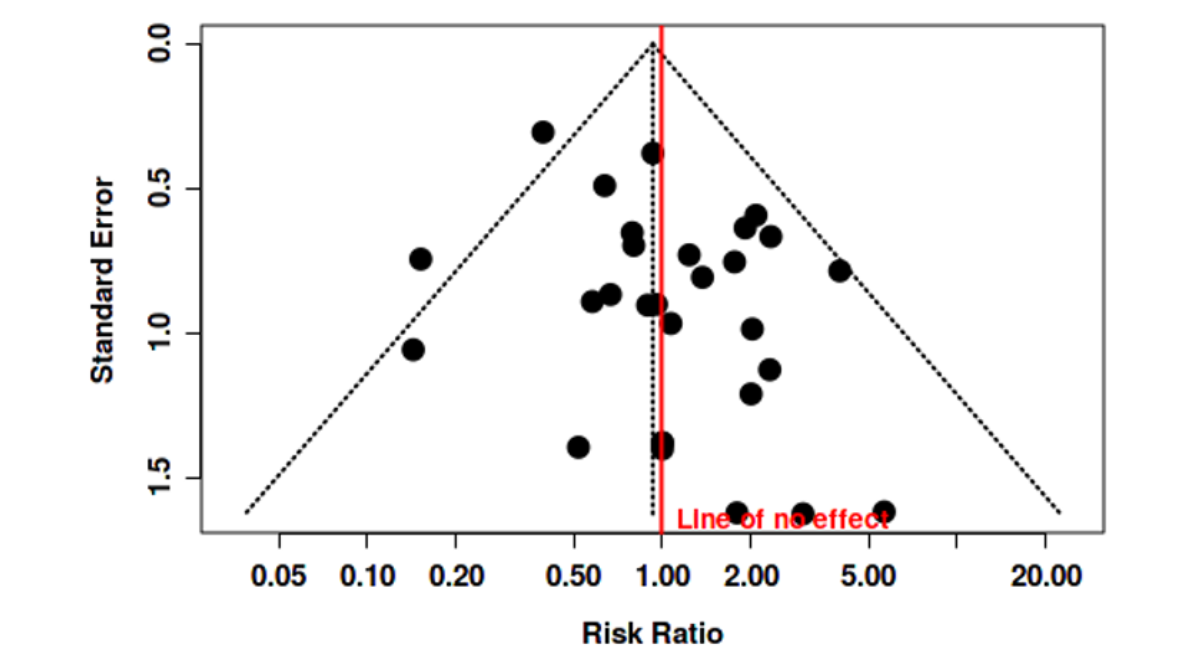
Figure S13: Funnel Plot Shows No Publication Bias Of EOA Between Stented And Stentless Group In Early Period (Intercept: 1.63, 95% CI: -2.1 - 5.36, T: 0.858, P-Value: 0.413).
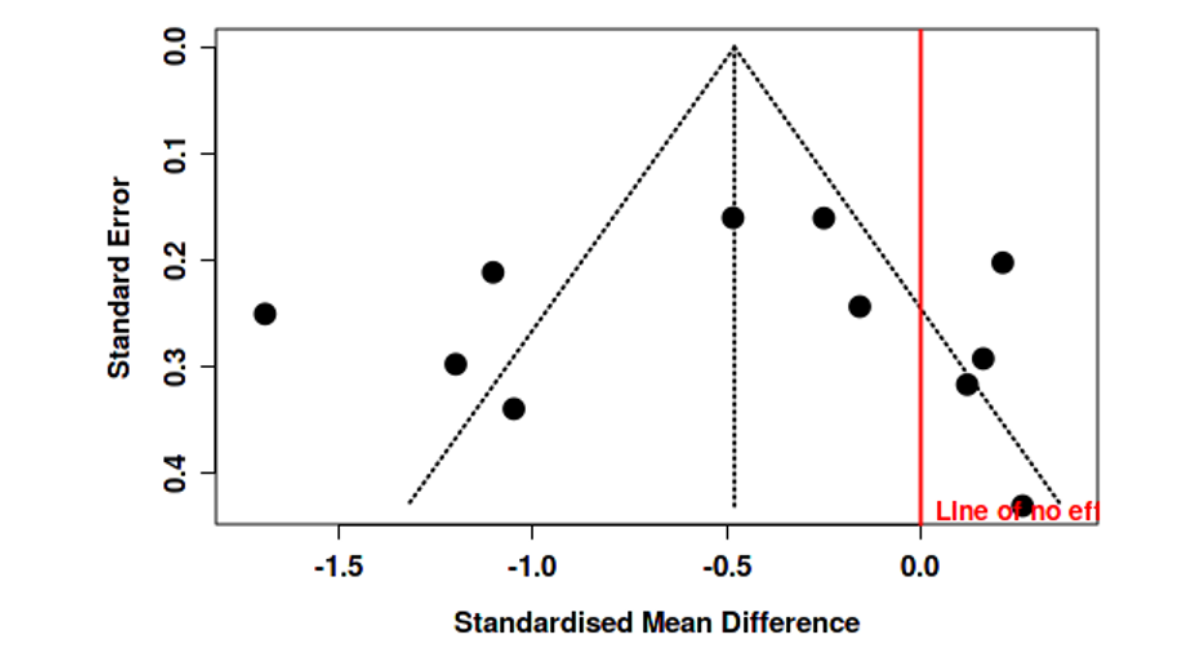
Figure S14: Funnel Plot Shows No Publication Bias of EOA Between Stented and Stentless Group in Late Period (Intercept: -0.47, 95% CI: -6.14 - 5.19, T: -0.164, P-Value: 0.874)
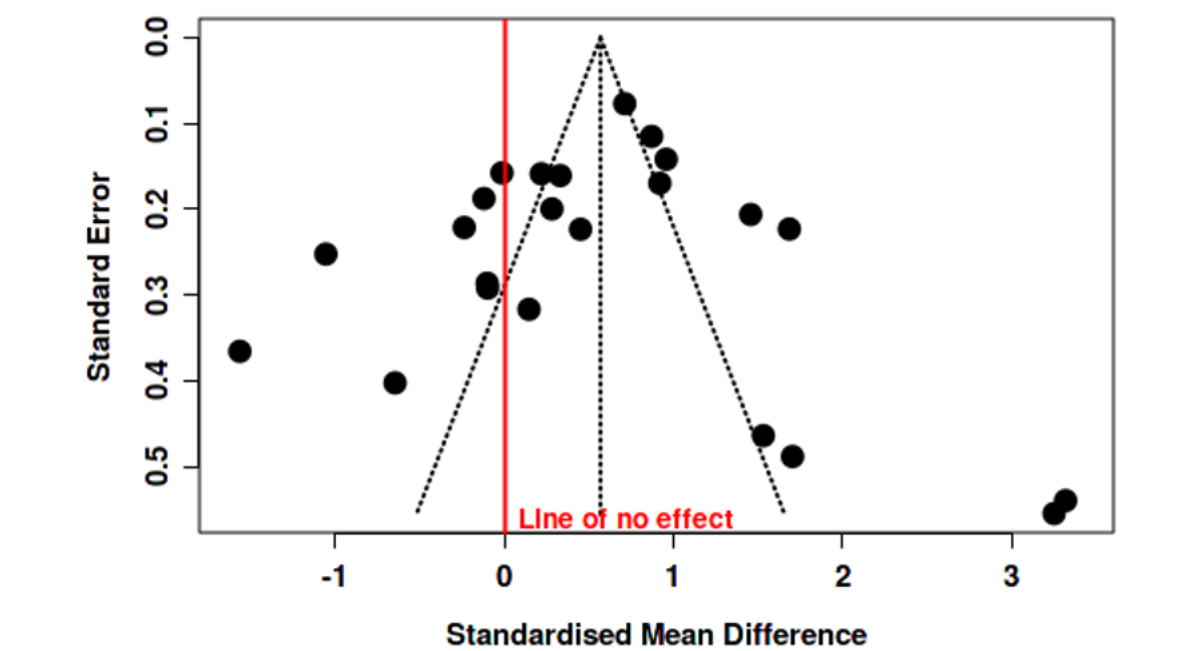
Figure S15: Funnel Plot Shows No Publication Bias of Transvalvular Mean Gradient Between Stented and Stentless Group in Early Period (Intercept: -0.6, 95% CI: -3.74 - 2.54, T: -0.373, P-Value: 0.713).
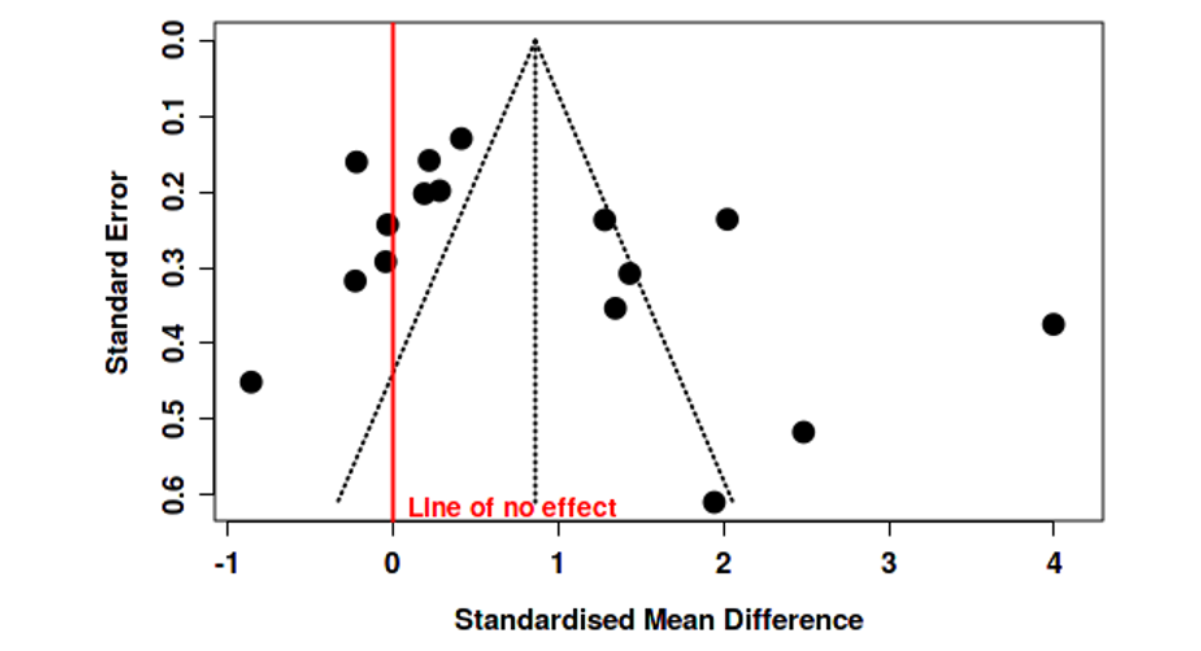
Figure S16: Funnel Plot Shows No Publication Bias of Transvalvular Mean Gradient Between Stented and Stentless Group in Late Period (Intercept: 4.34, 95% CI: -0.24 - 8.91, T: 1.859, P-Value: 0.084).
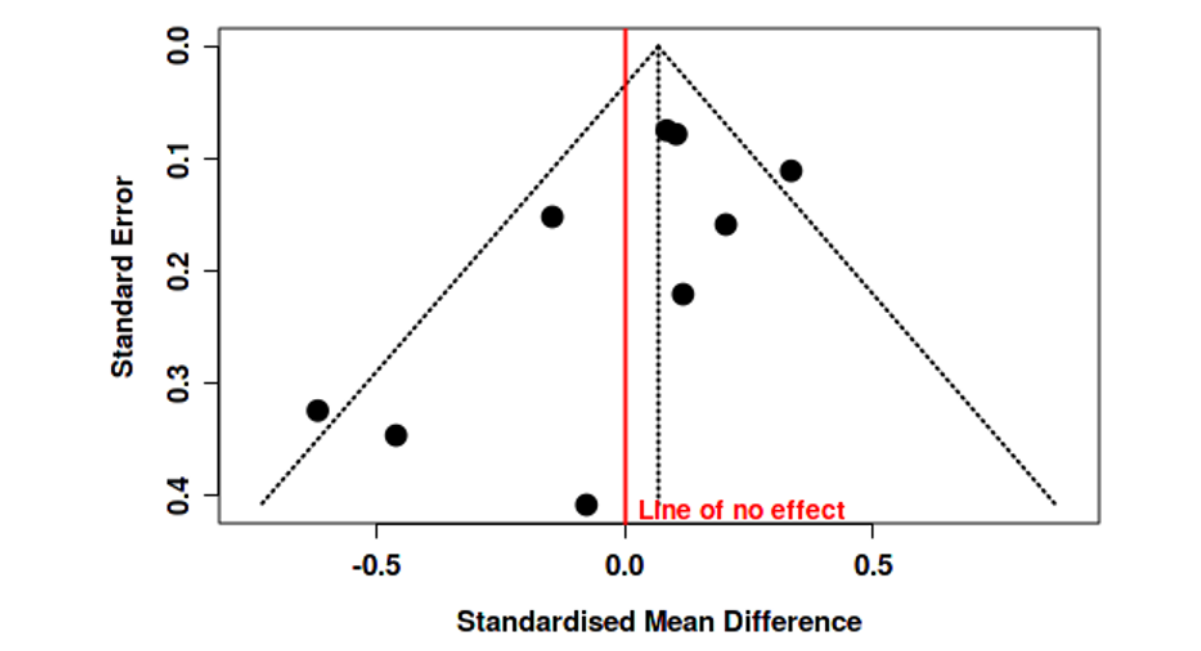
Figure S17: Funnel Plot Shows No Publication Bias of LVMR Between Stented and Stentless Group in Early Period (Intercept: -1.33, 95% CI: -2.99 - 0.33, T: -1.57, P-Value: 0.16).
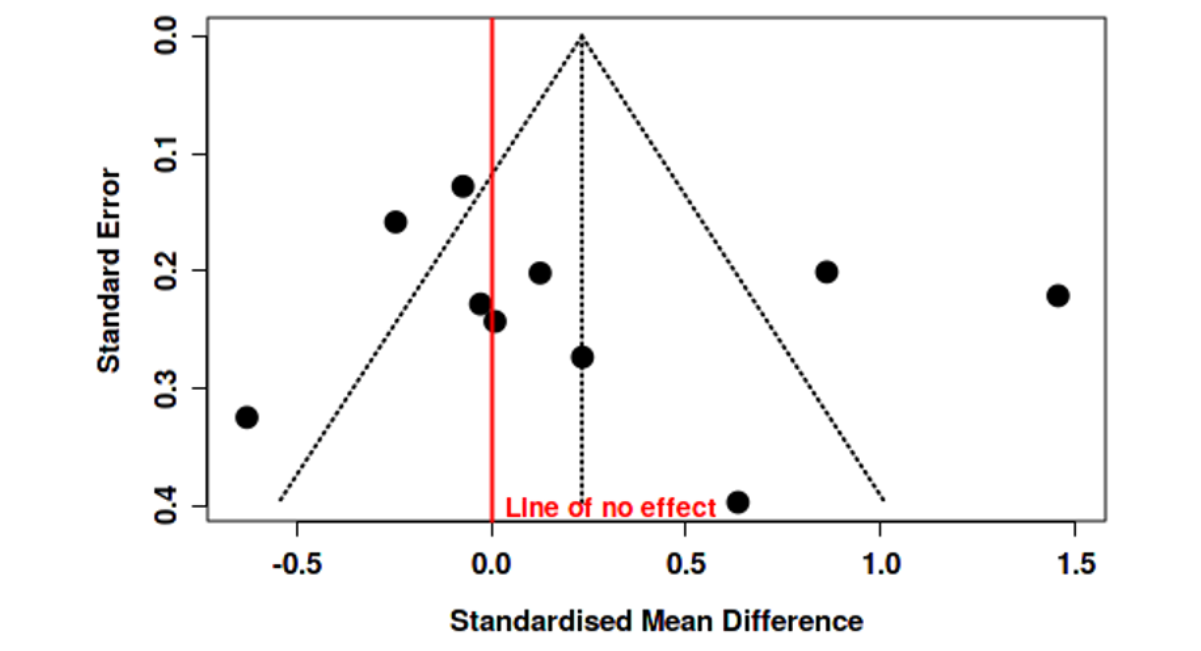
Figure S18: Funnel Plot Shows No Publication Bias of LVMR Between Stented and Stentless Group in Late Period (Intercept: 2, 95% CI: - 3.7 - 7.69, T: 0.686, P-Value: 0.512)
Quality Assessment
Risk of bias was assessed using the Newcastle-Ottawa scale (NOS) tool for cohort studies across three domains: selection, comparability and exposure. We also used Risk of Bias 2 (ROB2) for randomized studies which involves 5 domains: randomization process, deviation from intended interventions, missing outcome/s data, measurement of the outcome/s and selection of reported results. Responses to signaling questions in both tools were used to assign domain-level and over all bias judgments. (Supplementary Figure S19-20, Supplementary table 2).
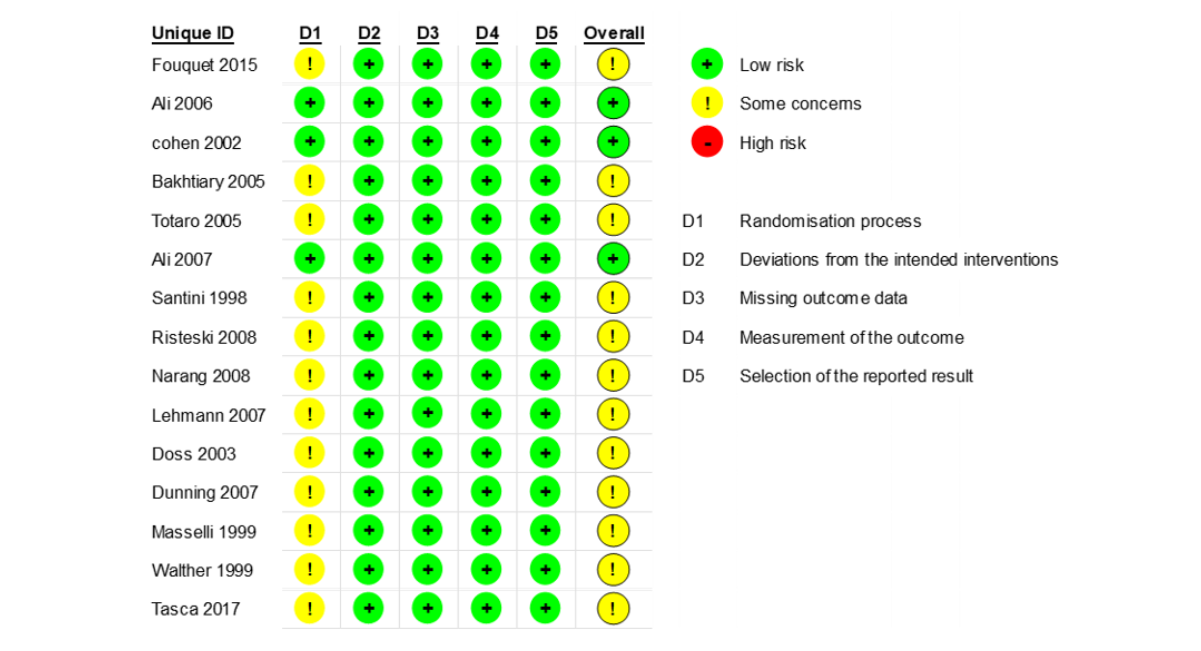
Figure S19: ROB CHECKLEST
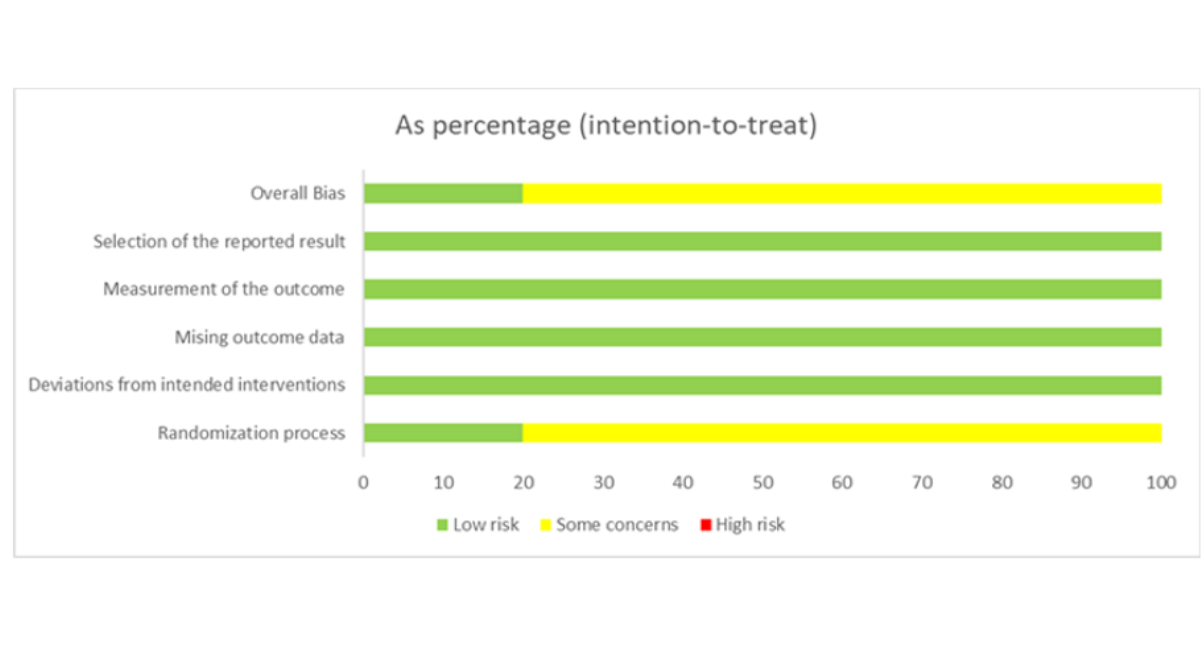
Figure S20: ROB chart
DISCUSSION
Aortic valve disease represents a major global health concern, affecting approximately 2–3% of the general population [11]. The management of this condition has evolved considerably over recent decades, with aortic valve replacement (AVR) remaining the cornerstone of treatment for severe disease [12]. Despite advancements in surgical techniques and prosthetic valve technology, the choice between stented and stentless bioprosthetic valves continues to be a subject of ongoing debate.
This meta-analysis compared the outcomes of stented and stentless aortic valve replacements in patients undergoing cardiac surgery. The pooled results indicate that stentless valves provide superior hemodynamic performance, characterized by larger effective orifice areas (EOA) and lower mean pressure gradients. However, our analysis did not demonstrate a statistically significant difference in left ventricular (LV) mass regression between the two valve types.
The hemodynamic advantages observed with stentless valves can be explained by their structural design. Unlike conventional stented prostheses, stentless valves lack a rigid supporting frame, allowing for a larger functional orifice and improved flow dynamics across the valve. This structural characteristic may reduce transvalvular gradients and improve ventricular unloading following surgery. Importantly, the observed hemodynamic superiority did not translate into measurable reductions in early mortality or major adverse clinical events.
These findings are in line with previous research demonstrating the hemodynamic advantages of stentless valves [13-15]. For instance, Dunning reported that stentless valves yielded lower transvalvular gradients and larger EOAs compared with stented prostheses, while Westaby observed improved hemodynamic efficiency and fewer valve-related complications in the stentless group [13,14].
However, our results also revealed no statistically significant differences in early all-cause mortality, stroke, myocardial infarction (MI), or endocarditis rates between the two valve types. This contrasts with certain earlier studies, such as Borow [16], which suggested a survival advantage with stentless valves. The discrepancies may be attributed to limitations in earlier studies, including small sample sizes, single-center designs, and short follow-up durations.
Subgroup analyses were conducted to explore potential sources of heterogeneity across the included studies. Differences in effect estimates between randomized controlled trials and observational studies may reflect variations in study design and patient selection. Observational studies are particularly susceptible to residual confounding and selection bias, which may influence the magnitude of the observed hemodynamic differences. In addition, variability between studies conducted before and after 2010 may reflect improvements in surgical techniques, perioperative management, and prosthetic valve design over time.
Although stentless valves demonstrated superior hemodynamic performance, these findings should not be interpreted as evidence supporting preferential use in specific patient populations, as pooled clinical outcomes remained comparable and the available evidence was predominantly observational. Conversely, stented valves might be better suited for older or higher-risk patients, where shorter operative times and technical simplicity are preferred. Moreover, the superior flow dynamics observed with stentless valves could translate into better exercise tolerance, symptom relief, and overall quality of life, although these benefits require confirmation in long-term follow-up studies [14,15].
Another important consideration is the potential for confounding by indication. In clinical practice, stentless valves are often selected for patients with small aortic annuli or those at risk of prosthesis patient mismatch, where maximizing the effective orifice area is particularly desirable. Consequently, baseline anatomical differences between treatment groups may influence the observed hemodynamic outcomes and limit the direct comparability between valve types in non-randomized studies.
Surgeon experience and familiarity with stentless implantation techniques may also influence operative outcomes and postoperative hemodynamics and represent potential sources of residual confounding that could not be evaluated in this meta-analysis.
Importantly, our results emphasize that valve selection should be individualized, considering patient age, anatomy, comorbidities, and life expectancy. Ongoing innovations, such as decellularized xenografts, polymeric valve materials, and minimally invasive implantation techniques, may further enhance the performance and durability of stentless prostheses, potentially expanding their clinical applicability.
Value and Importance of the Study
This meta-analysis contributes meaningfully to the growing body of evidence guiding the management of aortic valve disease. By systematically comparing the outcomes of stented and stentless valves, it provides clinicians and patients with an updated understanding of the trade-offs between hemodynamic superiority and procedural practicality. These insights can support more informed, patient-centered decision-making in clinical practice.
Furthermore, the study underscores the importance of careful patient selection and surgical planning in optimizing outcomes after AVR. It also identifies clear directions for future research, including the development of novel valve materials and designs, and the evaluation of long-term durability across different patient subgroups. Extended follow-up and real-world registry data will be crucial to validate these results and clarify the survival and quality-of-life implications of valve type.
Positioning against prior meta-analyses
Our findings are consistent with the foundational work of earlier meta-analyses, which established the hemodynamic superiority of stentless valves [64]. However, our study incorporates a substantially larger number of patients and more recent studies, strengthening the robustness of this conclusion. Furthermore, by adhering to PRISMA 2020 guidelines and employing comprehensive sensitivity analyses, we provide a methodologically rigorous update that confirms these hemodynamic benefits persist within the context of modern surgical practice and prosthesis design. In addition, our analysis evaluated perioperative clinical outcomes alongside hemodynamic parameters, providing a broader comparison between valve types than previous meta-analyses that focused primarily on hemodynamics.
Addressing long-term implications and ViV TAVI
A critical, unresolved question is whether the superior hemodynamics of stentless valves translate into improved long-term survival or durability. Our analysis, limited by the available literature, cannot answer this. The potential for enhanced left ventricular mass regression to confer a survival benefit is biologically plausible, but requires validation from long-term, prospective studies with standardized endpoints for structural valve degeneration.
Furthermore, the choice of bioprosthesis now must be considered within a lifetime management strategy for aortic valve disease. The advent of Valve-in-Valve (ViV) TAVI has transformed the approach to failed bioprostheses. In this context, the choice between a stented and stentless valve carries new implications. Stented valves provide a predictable, radiopaque landmark for ViV TAVI deployment. In contrast, stentless valves, particularly those implanted as a full root, can present a more complex anatomical substrate for ViV TAVI, potentially affecting coronary access and requiring advanced planning. Therefore, the decision must balance the desire for optimal initial hemodynamics against the future feasibility of transcatheter interventions, especially in younger patients likely to require a second procedure [65].
LIMITATIONS AND FUTURE DIRECTIONS
This meta-analysis has several limitations. Heterogeneity among the included studies was moderate to high for some outcomes, reflecting variations in patient selection, surgical techniques, and valve models. Additionally, publication bias was detected in the analyses of myocardial infarction and reoperation rates, which may have influenced the effect estimates.
While our analysis focused on early outcomes and hemodynamics, we systematically assessed the availability of long-term data on survival, structural valve degeneration, and reoperation. We found that the reporting of these outcomes was highly inconsistent across studies, with variable definitions, insufficient raw data, and a near-universal lack of patient-level time-to-event analyses (e.g., hazard ratios). Due to this significant heterogeneity and the high risk of bias in synthesizing absolute long-term rates from studies with differing follow-up durations, a formal meta-analysis of long-term outcomes was not feasible. This highlights a critical gap in the current literature.
Another practical limitation relates to the availability of stentless valves in certain healthcare systems. In some regions, including Jordan, stentless valves are not widely available, which may restrict their use even when theoretical clinical advantages exist.
Future studies with larger patient cohorts, standardized outcome definitions, and longer follow-up periods are essential to confirm these findings. Further research should also focus on predictors of valve durability, biomechanical performance, and next-generation stentless valve technologies [15,16].
CONCLUSION
In summary, this meta-analysis demonstrates that stentless aortic valves offer superior hemodynamic performance, reflected by larger EOAs and lower transvalvular gradients compared with stented valves. However, early mortality and major adverse event rates remain comparable between the two valve types. These findings underscore the importance of tailored valve selection in AVR and encourage continued innovation in valve design to further optimize patient outcomes.
ABBREVIATIONS
AVR: Aortic valve replacement
SAVR: Surgical aortic valve replacement
EOA: Effective orifice area
LV: Left ventricle
LVM: Left ventricular mass
CPB: Cardiopulmonary bypass
RR: Risk ratio
MD: Mean difference
CI: Confidence interval
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
FUNDING
No funding was received for this study.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
DATA AVAILABILITY
The data supporting the findings of this study are derived from previously published studies and are available in the public domain.
ETHICAL APPROVAL
This study was conducted using previously published data and did not involve human participants or animals.
ARTIFICIAL INTELLIGENCE DISCLOSURE
ChatGPT (OpenAI) was used solely for language editing and grammatical refinement. No artificial intelligence tools were used for study design, data extraction, statistical analysis, or interpretation of the results.
REFERENCES
- Cheng D, Pepper J, Martin J, Stanbridge R, Ferdinand FD, Jamieson WE, et al. Stentless versus stented bioprosthetic aortic valves: a systematic review and meta-analysis of controlled trials. Innovations. 2009;4(2):61-73. [Crossref] [Google Scholar] [PubMed]
- Dunning J, Graham RJ, Thambyrajah J, Stewart MJ, Kendall SW, Hunter S. Stentless vs. stented aortic valve bioprostheses: a prospective randomized controlled trial. European heart journal. 2007;28(19):2369-74. [Crossref] [Google Scholar] [PubMed]
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. New England Journal of Medicine. 1990;322(22):1561-6. [Crossref] [Google Scholar] [PubMed]
- Vrandecic M, Fantini FA, Filho BG, de Oliveira OC, da Costa Júnior IM, Vrandecic E. Retrospective clinical analysis of stented vs. stentless porcine aortic bioprostheses. European journal of cardio-thoracic surgery. 2000;18(1):46-53. [Crossref] [Google Scholar] [PubMed]
- Borger MA, Carson SM, Ivanov J, Rao V, Scully HE, Feindel CM, David TE. Stentless aortic valves are hemodynamically superior to stented valves during mid-term follow-up: a large retrospective study. The Annals of thoracic surgery. 2005;80(6):2180-5. [Crossref] [Google Scholar] [PubMed]
- Honos G, Cartier PC, Pibarot P, Dumesnil JG, Durand LG, Jobin J. Hemodynamic and physical performance during maximal exercise in patients with an aortic bioprosthetic valve: comparison of stentless versus stented bioprostheses. [Crossref] [Google Scholar]
- Aranda‐Michel E, Bianco V, Dufendach K, Kilic A, Habertheuer A, Humar R, et al. Midterm outcomes of subcoronary stentless porcine valve versus stented aortic valve replacement. Journal of Cardiac Surgery. 2020;35(11):2950-6. [Crossref] [Google Scholar] [PubMed]
- Khoo JP, Davies JE, Ang KL, Galiñanes M, Chin DT. Differences in performance of five types of aortic valve prostheses: haemodynamic assessment by dobutamine stress echocardiography. Heart. 2013;99(1):41-7. [Crossref] [Google Scholar] [PubMed]
- Jin XY, Gibson DG, Yacoub MH, Pepper JR. Perioperative assessment of aortic homograft, Toronto stentless valve, and stented valve in the aortic position. The Annals of thoracic surgery. 1995 ;60:S395-401. [Crossref] [Google Scholar] [PubMed]
- Lehmann S, Walther T, Kempfert J, Leontyev S, Bakhtiary F, Rastan A, Mohr FW. Ten-year follow up after prospectively randomized evaluation of stentless versus conventional xenograft aortic valve replacement. The Journal of Heart Valve Disease. 2011;20(6):681-7. [Google Scholar] [PubMed]
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. The lancet. 2006;368(9540):1005-11. [Crossref] [Google Scholar] [PubMed]
- Kobayashi J. Stentless aortic valve replacement: an update. Vascular health and risk management. 2011:345-51. [Crossref] [Google Scholar] [PubMed]
- Dunning J, Graham RJ, Thambyrajah J, Stewart MJ, Kendall SW, Hunter S. et al. stented aortic valve bioprostheses: a prospective randomized controlled trial. European heart journal. 2007;28(19):2369-74. [Crossref] [Google Scholar] [PubMed]
- Ennker J, Albert A, Ennker IC. Stentless aortic valves. Current aspects. HSR proceedings in intensive care & cardiovascular anesthesia. 2012;4(2):77. [Google Scholar] [PubMed]
- Kobayashi J. Stentless aortic valve replacement: an update. Vascular health and risk management. 2011:345-51. [Crossref] [Google Scholar] [PubMed]
- Tavakoli R, Danial P, Oudjana AH, Jamshidi P, Gassmann M, Leprince P, et al. Biological aortic valve replacement: advantages and optimal indications of stentless compared to stented valve substitutes. A review. General thoracic and cardiovascular surgery. 2018;66(5):247-56. [Crossref] [Google Scholar] [PubMed]
- Bové T, Van Belleghem Y, François K, Caes F, Van Overbeke H, Van Nooten G. Stentless and stented aortic valve replacement in elderly patients: factors affecting midterm clinical and hemodynamical outcome. European journal of cardio-thoracic surgery. 2006;30(5):706-15. [Crossref] [Google Scholar] [PubMed]
- Brown ML, Park SJ, Sundt TM, Schaff HV. Early thrombosis risk in patients with biologic valves in the aortic position. The Journal of thoracic and cardiovascular surgery. 2012;144(1):108-11. [Crossref] [Google Scholar] [PubMed]
- Burgazli KM, Mericliler M, Erenturk S, Polat ZP, Atmaca N. Early postoperative hemodynamic performances of stented versus stentless aortic xenografts in aortic valve replacement in elderly patients: a comparative study. European Review for Medical & Pharmacological Sciences. 2013;17(14). [Crossref] [Google Scholar] [PubMed]
- Casabona R, De Paulis R, Zattera GF, di Summa M, Bottone W, Stacchino C, et al. Stenless porcine and pericardial valve in aortic position. The Annals of thoracic surgery. 1992;54(4):681-5. [Crossref] [Google Scholar] [PubMed]
- Choi CH, Cheng V, Malaver D, Kon N, Kincaid EH, Gandhi SK, Applegate RJ, Zhao DX. A comparison of valve‐in‐valve transcatheter aortic valve replacement in failed stentless versus stented surgical bioprosthetic aortic valves. Catheterization and Cardiovascular Interventions. 2019;93(6):1106-15. [Crossref] [Google Scholar] [PubMed]
- Christ T, Holinski S, Zhigalov K, Zielinski CB, Grubitzsch H. Hemodynamics of pericardial aortic valves: contemporary stented versus stentless valves in a matched comparison. Annals of Thoracic and Cardiovascular Surgery. 2017;23(6):298-303. [Crossref] [Google Scholar] [PubMed]
- Totaro P, Degno N, Zaidi A, Youhana A, Argano V. Carpentier-Edwards PERIMOUNT Magna bioprosthesis: a stented valve with stentless performance?. The Journal of Thoracic and Cardiovascular Surgery. 2005;130(6):1668-74. [Crossref] [Google Scholar] [PubMed]
- Clemence Jr J, Caceres J, Ren T, Wu X, Kim KM, Patel HJ, Deeb GM, Yang B. Treatment of aortic valve endocarditis with stented or stentless valve. The Journal of thoracic and cardiovascular surgery. 2022;164(2):480-7. [Crossref] [Google Scholar] [PubMed]
- Cohen G, Christakis GT, Joyner CD, Morgan CD, Tamariz M, Hanayama N, et al. Are stentless valves hemodynamically superior to stented valves? A prospective randomized trial. The Annals of thoracic surgery. 2002;73(3):767-78. [Crossref] [Google Scholar] [PubMed]
- Narang S, Satsangi DK, Banerjee A, Geelani MA. Stentless valves versus stented bioprostheses at the aortic position: midterm results. The Journal of Thoracic and Cardiovascular Surgery. 2008 Oct 1;136(4):943-7. [Crossref] [Google Scholar] [PubMed]
- Fouquet O, Baufreton C, Tassin A, Pinaud F, Binuani JP, DangVan S, et al. Influence of stentless versus stented valves on ventricular remodeling assessed at 6 months by magnetic resonance imaging and long-term follow-up. Journal of Cardiology. 2017;69(1):264-71. [Crossref] [Google Scholar] [PubMed]
- Ali A, Halstead JC, Cafferty F, Sharples L, Rose F, Lee E, et al. Early clinical and hemodynamic outcomes after stented and stentless aortic valve replacement: results from a randomized controlled trial. The Annals of thoracic surgery. 2007;83(6):2162-8. [Crossref] [Google Scholar] [PubMed]
- Bakhtiary F, Schiemann M, Dzemali O, Dogan S, Schächinger V, Ackermann H, et al. Impact of patient-prosthesis mismatch and aortic valve design on coronary flow reserve after aortic valve replacement. Journal of the American College of Cardiology. 2007;49(7):790-6. [Crossref] [Google Scholar] [PubMed]
- Böning A, Niemann B, Ennker I, Richter M, Roth P, Ennker J. Are aortic valve reoperations after primary replacement with stentless heart valve prostheses more demanding than after stented biological prostheses?. The Thoracic and cardiovascular surgeon. 2014;62(06):475-81. [Crossref] [Google Scholar] [PubMed]
- Cerqueira RJ, Raimundo R, Moreira S, Saraiva FA, Andrade M, Salgueiro E, et al. Freedom Solo® versus Trifecta® bioprostheses: clinical and haemodynamic evaluation after propensity score matching. European Journal of Cardio-Thoracic Surgery. 2018;53(6):1264-71. [Crossref] [Google Scholar] [PubMed]
- Ali A, Halstead JC, Cafferty F, Sharples L, Rose F, Coulden R, et al. Are stentless valves superior to modern stented valves? A prospective randomized trial. Circulation. 2006;114(1_supplement):I-535. [Crossref] [Google Scholar] [PubMed]
- David TE, Puschmann R, Ivanov J, Bos J, Armstrong S, et al. Aortic valve replacement with stentless and stented porcine valves: a case-match study. The Journal of Thoracic and Cardiovascular Surgery. 1998;116(2):236-41. [Crossref] [Google Scholar] [PubMed]
- Collinson J, Henein M, Flather M, Pepper JR, Gibson DG. Valve replacement for aortic stenosis in patients with poor left ventricular function: comparison of early changes with stented and stentless valves. Circulation. 1999;100(19):II-5. [Crossref] [Google Scholar] [PubMed]
- Christakis GT, Joyner CD, Morgan CD, Fremes SE, Buth KJ, Sever JY, et al. Left ventricular mass regression early after aortic valve replacement. The Annals of thoracic surgery. 1996;62(4):1084-9. [Crossref] [Google Scholar] [PubMed]
- Dossche K, Vanermen H, Wellens F, De Geest R, Degrieck I, Deloof T. Free-hand sewn allografts, stentless (Prima Edwards) and stented (CESA) porcine bioprostheses. European journal of cardio-thoracic surgery. 1995;9(10):562-7. [Crossref] [Google Scholar] [PubMed]
- Dumesnil JG, LeBlanc MH, Cartier PC, Métras J, Desaulniers D, Doyle DP, et al. Hemodynamic features of the freestyle aortic bioprosthesis compared with stented bioprosthesis. The Annals of thoracic surgery. 1998;66(6):S130-3. [Crossref] [Google Scholar] [PubMed]
- Doss M, Martens S, Wood JP, Aybek T, Kleine P, Wimmer Greinecker G, et al. Performance of stentless versus stented aortic valve bioprostheses in the elderly patient: a prospective randomized trial. European journal of cardio-thoracic surgery. 2003;23(3):299-304. [Crossref] [Google Scholar] [PubMed]
- Collinson J, Flather M, Coats AJ, Pepper JR, Henein M. Influence of valve prosthesis type on the recovery of ventricular dysfunction and subendocardial ischaemia following valve replacement for aortic stenosis. International journal of cardiology. 2004;97(3):535-41. [Crossref] [Google Scholar] [PubMed]
- Hirnle T, Juszczyk G, Tycińska A, Stankiewicz A, Żak G, Lewczuk A, et al. Trombocytopenia i powikłania okołooperacyjne po implantacji biologicznej protezy bezstentowej Freedom Solo. Kardiologia Polska. 2013;71(4). [Crossref] [Google Scholar] [PubMed]
- Jin XY, Gibson DG, Yacoub MH, Pepper JR. Perioperative assessment of aortic homograft, Toronto stentless valve, and stented valve in the aortic position. The Annals of thoracic surgery. 1995;60:S395-401. [Crossref] [Google Scholar] [PubMed]
- Hegazy YY, Rayan A, Sodian R, Hassanein W, Ennker J. Medtronic Freestyle aortic bioprosthesis: a potential option for haemodialysis patients. Interactive cardiovascular and thoracic surgery. 2016;22(4):459-64. [Crossref] [Google Scholar] [PubMed]
- Maselli D, Pizio R, Bruno LP, Di Bella I, De Gasperis C . Left ventricular mass reduction after aortic valve replacement: homografts, stentless and stented valves. The Annals of thoracic surgery. 1999;67(4):966-71. [Crossref] [Google Scholar] [PubMed]
- Milano AD, Blanzola C, Mecozzi G, D’Alfonso A, De Carlo M, Nardi C, Bortolotti U. Hemodynamic performance of stented and stentless aortic bioprostheses. The Annals of thoracic surgery. 2001;72(1):33-8. [Crossref] [Google Scholar] [PubMed]
- Murashita T, Okada Y, Kanemitsu H, Fukunaga N, Konishi Y, Nakamura K, Koyama T. Efficacy of stentless aortic bioprosthesis implantation for aortic stenosis with small aortic annulus. The Thoracic and cardiovascular surgeon. 2015;63(06):446-51. [Crossref] [Google Scholar] [PubMed]
- Rao V, Christakis GT, Sever J, Fremes SE, Bhatnagar G, Cohen G, et al. A novel comparison of stentless versus stented valves in the small aortic root. The Journal of Thoracic and Cardiovascular Surgery. 1999;117(3):431-8. [Crossref] [Google Scholar] [PubMed]
- Tamim M, Bové T, Van Belleghem Y, François K, Taeymans Y, Van Nooten GJ. Stentless vs. stented aortic valve replacement: left ventricular mass regression. Asian Cardiovascular and Thoracic Annals. 2005;13(2):112-8. [Crossref] [Google Scholar] [PubMed]
- Tsialtas D, Bolognesi R, Beghi C, Albertini D, Bolognesi MG, Manca C, Gherli T. Stented versus stentless bioprostheses in aortic valve stenosis: effect on left ventricular remodelling. InThe Heart Surgery Forum 2007(Vol. 10, No. 3, pp. 205-210). IMR Press. [Crossref] [Google Scholar] [PubMed]
- Tsialtas D, Bolognesi R, Beghi C, Albertini D, Bolognesi MG, Manca C, Gherli T. Stented versus stentless bioprostheses in aortic valve stenosis: effect on left ventricular remodelling. InThe Heart Surgery Forum 2007(Vol. 10, No. 3, pp. 205-210). IMR Press. [Crossref] [Google Scholar] [PubMed]
- Van Nooten G, Caes F, François K, Van Belleghem Y, Taeymans Y. Stentless or stented aortic valve implants in elderly patients?. European journal of cardio-thoracic surgery. 1999;15(1):31-6. [Crossref] [Google Scholar] [PubMed]
- Walther T, Falk V, Langebartels G, Krüger M, Bernhardt U, Diegeler A, et al. Prospectively randomized evaluation of stentless versus conventional biological aortic valves: impact on early regression of left ventricular hypertrophy. Circulation. 1999;100(19):II-10. [Crossref] [Google Scholar] [PubMed]
- Konertz J, Zhigalov K, Weymann A, Dohmen PM. Initial experience with aortic valve replacement via a minimally invasive approach: a comparison of stented, stentless and sutureless valves. Medical science monitor: international medical journal of experimental and clinical research. 2017;23:1645. [Crossref] [Google Scholar] [PubMed]
- Kunihara T, Schmidt K, Glombitza P, Dzindzibadze V, Lausberg H, Schäfers HJ. Root replacement using stentless valves in the small aortic root: a propensity score analysis. The Annals of thoracic surgery. 2006;82(4):1379-84. [Crossref] [Google Scholar] [PubMed]
- Risteski PS, Martens S, Rouhollahpour A, Wimmer-Greinecker G, Moritz A, et al. Prospective randomized evaluation of stentless vs. stented aortic biologic prosthetic valves in the elderly at five years. Interactive cardiovascular and thoracic surgery. 2009;8(4):449-53. [Crossref] [Google Scholar] [PubMed]
- Schaefer A, Dickow J, Schoen G, Westhofen S, Kloss L, Al-Saydali T, et al. Stentless vs. stented bioprosthesis for aortic valve replacement: a case matched comparison of long-term follow-up and subgroup analysis of patients with native valve endocarditis. PloS one. 2018;13(1):e0191171. [Google Scholar] [PubMed]
- Wollersheim LW, Li WW, Kaya A, Bouma BJ, Driessen AH, van Boven WJ, et al. Stentless vs stented aortic valve bioprostheses in the small aortic root. InSeminars in Thoracic and Cardiovascular Surgery 2016 (Vol. 28, No. 2, pp. 390-397). WB Saunders. [Crossref] [Google Scholar] [PubMed]
- Yang B, Makkinejad A, Fukuhara S, Clemence Jr J, Farhat L, Malik A, Wu X, Kim K, Patel H, Deeb GM. Stentless versus stented aortic valve replacement for aortic stenosis. The Annals of thoracic surgery. 2022;114(3):728-34. [Crossref] [Google Scholar] [PubMed]
- Stefanelli G, Pirro F, Smorto V, Bellisario A, Chiurlia E, Weltert L. Stentless Pericarbon Freedom Versus Stented Perimount Aortic Bioprosthesis: Propensity-Matched Long-Term Follow-Up. Innovations. 2020;15(5):440-8. [Crossref] [Google Scholar] [PubMed]
- Tasca G, Vismara R, Trinca F, Riva B, Gamba A, Lobiati E. Opening/closing pattern of Trifecta and Freestyle valves versus native aortic valve: Are stentless valves more physiologic than a stented valve?. Journal of Cardiac Surgery. 2017;32(11):680-5. [Crossref] [Google Scholar] [PubMed]
- Santini F, Bertolini P, Montalbano G, Vecchi B, Pessotto R, Prioli A, et al. Hancock versus stentless bioprostheses for aortic valve replacement in patients older than 75 years. The Annals of thoracic surgery. 1998 Dec 1;66(6):S99-103. [Crossref] [Google Scholar] [PubMed]
- Chambers J, Rimington H, Rajani R, Hodson F, Blauth C. Hemodynamic performance on exercise: comparison of a stentless and stented biological aortic valve replacement. Journal of Heart Valve Disease. 2004;13(5):729-33. [Crossref] [Google Scholar] [PubMed]
- De Paulis R, Sommariva L, Colagrande L, De Matteis GM, Fratini S, Tomai F, et al. Regression of left ventricular hypertrophy after aortic valve replacement for aortic stenosis with different valve substitutes. The Journal of Thoracic and Cardiovascular Surgery. 1998;116(4):590-8. [Crossref] [Google Scholar] [PubMed]
- Luciani GB, Casali G, Auriemma S, Santini F, Mazzucco A. Survival after stentless and stented xenograft aortic valve replacement: a concurrent, controlled trial. The Annals of thoracic surgery. 2002;74(5):1443-9. [Crossref] [Google Scholar] [PubMed]
- Cheng D, Pepper J, Martin J, Stanbridge R, Ferdinand FD, Jamieson WE, Stelzer P, Berg G, Sani G. Stentless versus stented bioprosthetic aortic valves: a systematic review and meta-analysis of controlled trials. Innovations. 2009;4(2):61-73. [Crossref] [Google Scholar]
- Dvir D, Webb JG, Bleiziffer S, Pasic M, Waksman R, Kodali S, et al. Transcatheter aortic valve implantation in failed bioprosthetic surgical valves. Jama. 2014;312(2):162-70. [Crossref] [Google Scholar] [PubMed]
{kind=link}
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 25-35 Days |
Peer Review Feedback |
| 45-60 Days | Total article processing time |
Ethics & Policies
Editorial & Management
Useful Links
Journal Highlights
Open Access Journals
Journal Flyer