Journal of Psychiatry and Psychological Sciences
ISSN:
3107-9024 (Online)
DOI Prefix (Crossref): 10.67238
ABSTRACT
Background
Attachment theory has provided one of the most influential frameworks for understanding early relational development, affect regulation, and later interpersonal functioning. Foundational work by Bowlby, Ainsworth, Main, and subsequent attachment researchers has clarified how early caregiving shapes relational expectations and behavioural patterns. However, attachment classifications alone may not fully explain the deeper structural mechanisms through which early relational experience becomes internal object organisation, predictive affect regulation, personality formation, and vulnerability to collapse under relational stress.
Aim
This paper introduces the Anticipatory Stress Reflex Complex, or ASR Complex, within Mirrored Psychic Inversion Theory as a proposed integrative framework for understanding attachment, personality development, trauma response, and internal object formation.
Methods
The paper uses an integrative narrative review and conceptual synthesis. It draws on attachment theory, objects relations, affect regulation, developmental trauma, mentalisation, predictive processing, interoception, personality organisation, and selected literature on collapse and near-death phenomenology. The aim is theoretical integration rather than meta-analysis or empirical testing.
Conceptual findings
The ASR Complex is proposed as a tripartite organising architecture comprising ASR1, the primordial affective field; ASR3, the unconscious internal object world; and ASR2, the mature predictive ego and reality-mediating gate. Within this model, attachment styles are reframed as behavioural expressions of deeper ASR configurations, while personality organisation is conceptualised as the stabilised adult form of early ASR development.
Conclusion
The ASR Complex may offer a clinically useful structural language for linking attachment, affect regulation, internal object relations, predictive self-organisation, trauma, and personality development. Further empirical, longitudinal, neurobiological, and clinical validation is required.
Keywords: Anticipatory Stress Reflex; ASR Complex; Attachment Theory; Personality Development; Object Relations; Affect Regulation; Predictive Processing; Developmental Trauma; MPIT
INTRODUCTION
Attachment theory remains one of the central organising frameworks in developmental psychology, clinical psychology, and relational psychoanalysis. Since Bowlby’s formulation of attachment as a biologically grounded behavioural system and Ainsworth’s observational studies of infant-caregiver interaction, attachment research has provided an enduring language for understanding proximity-seeking, separation distress, secure-base behaviour, and the development of internal working models [1-4]. Later work by Main and Solomon extended the field by identifying disorganised attachment, clarifying how frightening, frightened, or unresolved caregiving may produce contradictory behavioural strategies in the child [5].
The strength of attachment theory lies in its capacity to describe observable relational patterns and their developmental consequences. Secure, anxious, avoidant, and disorganised configurations remain clinically useful because they capture recurring relational strategies across infancy, childhood, adult intimacy, and therapeutic process. Contemporary research continues to demonstrate the relevance of attachment insecurity to emotion regulation, interpersonal functioning, psychopathology, and therapeutic alliance [6,7].
However, a persistent conceptual problem remains. Attachment classifications describe patterns of behaviour, affect regulation, and relational expectation, but they do not fully specify the deeper structural mechanism through which early caregiving experience becomes stable internal organisation.
Mirrored Psychic Inversion Theory proposes the Anticipatory Stress Reflex Complex, hereafter ASR Complex, as a theoretical model for addressing this structural gap [8]. The ASR Complex is not presented as a replacement for attachment theory, object relations, trauma theory, or predictive processing. Rather, it is proposed as an integrative framework through which these traditions may be brought into a single developmental and clinical architecture. The model argues that attachment style is not merely a behavioural disposition, but the visible relational signature of a deeper organising system involving affective vulnerability, internalised object relations, predictive modelling, and reality mediation.
The ASR Complex is organised around three proposed layers: ASR1, ASR3, and ASR2. ASR1 refers to the primordial affective field: the infant’s earliest somatic, pre-symbolic vulnerability and dependence on external regulation. ASR3 refers to the symbolic unconscious or internal object world: the implicit relational architecture formed through repeated caregiver interactions, introjects, shame states, threat templates, and expectations of safety or rupture. ASR2 refers to the conscious predictive ego: the mature, reality-mediating function capable of symbolic delay, object constancy, reflective processing, affect regulation, and self-other differentiation.
This paper argues that contemporary developments in developmental neuroscience, trauma studies, affect regulation theory, mentalisation research, interoception, and predictive processing provide an opportunity to revisit attachment theory at a structural level. The brain is increasingly understood not as a passive receiver of external information but as an anticipatory, prediction-generating organ that regulates perception, affect, and action through embodied inference [9-13]. Complex trauma research similarly suggests that prolonged relational threat may alter self-organisation, affect regulation, interpersonal expectation, and embodied [14]. These developments allow attachment to be reconsidered not simply as behaviour, but as the outcome of a layered regulatory architecture. The purpose of this paper is therefore to present the ASR Complex as an integrative review and conceptual synthesis linking attachment, object relations, and affect regulation, predictive processing, developmental trauma, collapse vulnerability, and personality organisation. The paper does not claim that the ASR Complex has yet been empirically validated. Rather, it proposes a theoretical model requiring further operationalisation, measurement, and clinical testing.
Problem Statement
Current attachment models have been highly valuable in describing relational patterns, developmental trajectories, and characteristic responses to proximity, rupture, threat, and repair. However, they do not fully explain the structural mechanism through which early caregiving experience becomes internal object organisation, predictive affect regulation, personality structure, collapse vulnerability, and treatment resistance.
This limitation is particularly visible when attachment categories are used descriptively without a deeper account of the internal architecture that generates them. A person may be described as anxious, avoidant, disorganised, dependent, narcissistic, borderline, schizoid, echoistic, or fearful, yet these labels do not by themselves explain how early affective experience, internalised objects, embodied prediction, shame, splitting, and self-continuity become organised into a stable personality pattern.
MPIT proposes that the ASR Complex may function as a missing structural mechanism. It offers a layered model through which attachment behaviour can be understood as the surface expression of deeper affective, object-relational, and predictive organisation.
Method: Integrative Narrative Review and Conceptual Synthesis
This paper uses an integrative narrative review and conceptual synthesis. It does not present an empirical study, statistical analysis, systematic review, or meta-analysis. Its method is interpretive and theoretical: it draws together established bodies of literature and maps their conceptual convergences through the proposed ASR Complex.
The review draws on several domains: attachment theory, object relations, developmental trauma, affect regulation, mentalisation and reflective function, predictive processing and active inference, interoception, personality organisation, and selected literature on near-death and collapse phenomenology. The inclusion of collapse and near-death literature is cautious and comparative. It is used to support conceptual thinking about self-dissolution, consciousness, and regression, not as direct proof of the ASR model.
The synthesis proceeds by comparative theoretical mapping. First, attachment theory is reviewed as the behavioural and relational foundation. Second, object relations theory is used to account for internal object formation, splitting, introjection, false self organisation, and object constancy. Third, developmental trauma and mentalisation literatures are used to examine affect regulation, reflective capacity, dissociation, and self-organisation under relational threat. Fourth, predictive processing and interoceptive inference are used to situate the ASR Complex within contemporary models of the anticipatory brain. Finally, personality organisation is considered as a stabilised structural outcome of early relational, affective, and predictive development.
The limitations of this method must be stated clearly. The ASR Complex remains a conceptual model. It requires operationalisation, empirical testing, longitudinal validation, and clinical outcome research. The value of the present paper lies in theoretical integration and hypothesis generation rather than empirical confirmation.
Literature Review
Attachment Theory and Internal Working Models
Attachment theory began with Bowlby’s claim that infants are biologically predisposed to seek proximity to caregivers under conditions of threat, distress, or separation [2-4]. Ainsworth extended this theory through observational research, identifying secure, avoidant, and resistant or ambivalent attachment patterns in the Strange Situation Procedure [1]. Main and Solomon later identified disorganised attachment, characterised by contradictory, disoriented, or apprehensive behaviours in the presence of the caregiver [5].
The concept of internal working models is particularly important for the present paper. Bowlby proposed that repeated caregiver interactions become internalised as expectations about the self, others, and the availability of care. These models are not merely cognitive beliefs; they are affective and relational templates that shape perception, anticipation, and behaviour. Contemporary attachment research continues to explore how attachment security and insecurity influence emotion regulation, interpersonal functioning, autobiographical memory, and psychological distress [6,7]. However, attachment theory often moves from observed behaviour to inferred internal models without fully specifying the deeper architecture by which those models become organised, defended, and stabilised. The ASR Complex builds upon attachment theory by proposing that attachment behaviours emerge from a layered system involving primordial affective vulnerability, unconscious internal object organisation, and conscious predictive mediation.
Object Relations and Internal Object Formation
Object relations theory provides a second foundation for the ASR Complex. Fairbairn shifted psychoanalytic emphasis from drives to relationships, arguing that the infant’s primary motivation is object-seeking rather than pleasure-seeking [15]. His model of the endopsychic structure, including libidinal and anti-libidinal ego positions, offers an important framework for understanding how internal objects become organised around longing, rejection, attachment, and defensive hostility.
Klein described splitting, projective identification, and the movement between paranoid-schizoid and depressive positions [16]. Her work clarifies how early psychic life may divide objects into good and bad when ambivalence cannot yet be tolerated. Winnicott introduced the true self and false self distinction, emphasising the role of the facilitating environment and the caregiver’s capacity to meet the infant’s spontaneous gesture [17,18]. Where the environment fails repeatedly, the child may develop a compliant false self to protect the vulnerable true self.
Kernberg later integrated object relations with personality organisation, particularly in relation to borderline and narcissistic structures. His work on identity diffusion, splitting, primitive defences, and object constancy remains central to understanding personality pathology as structural rather than merely symptomatic [19,20].
The ASR Complex incorporates these traditions by locating internal objects primarily within ASR3. ASR3 is proposed as the unconscious relational blueprint: the internal object world through which the child carries implicit expectations of safety, abandonment, shame, engulfment, hostility, or repair. In this model, attachment style is not only a behavioural pattern; it is an ASR2 strategy built upon ASR3 object relations and designed to regulate ASR1 vulnerability.
Affect Regulation, Developmental Trauma, and Mentalisation
Affect regulation is central to attachment development. Schore argued that early right-brain development is shaped by caregiver regulation, especially through affective attunement, gaze, facial expression, rhythm, and repair [21,22]. Van der Kolk similarly emphasised that trauma is not merely remembered cognitively but carried somatically, shaping arousal, dissociation, threat response, and self-experience [23].
Fonagy later mentalisation-based approaches place reflective function at the centre of psychological development [24]. Mentalisation allows the child to understand self and other in terms of intentional mental states. Trauma, especially when inflicted or mediated by attachment figures, may impair reflective capacity, disrupt affect regulation, and produce defensive certainty, dissociation, or collapse under relational stress [25].
Complex trauma literature increasingly recognises that prolonged relational threat is associated not only with fear-based symptoms, but with disturbances in self-organisation, affect regulation, relational functioning, and negative self-concept [15]. This is highly relevant to the ASR model. MPIT proposes that chronic misattunement, humiliation, abandonment, coercion, or frightening caregiving may alter not only behaviour but the organising architecture through which affect and reality are mediated.
Predictive Processing, Interoception, and Active Inference
Predictive processing and active inference provide a contemporary mechanism for understanding the mind as anticipatory rather than merely reactive. Friston proposed that the brain minimises prediction error by generating models of the causes of sensory input [10]. Hohwy and Clark further developed the view of the brain as a prediction-generating system [9-11]. Barrett emphasised the role of interoception and allostasis in emotion construction, while Seth and Friston linked selfhood and consciousness to embodied predictive regulation.
Recent predictive processing models have also been applied to affective neuroscience and trauma. Lee and colleagues argued that predictive processing offers a useful framework for understanding affective and cognitive neuroscience [26]. Putica proposed a predictive-processing interpretation of complex post-traumatic stress disorder, linking disturbances in self-organisation to altered prediction, affect regulation, and interpersonal expectation. The ASR Complex is compatible with this anticipatory view of mind. ASR2 can be understood as the mature predictive ego: the layer capable of modulating uncertainty, tolerating ambiguity, updating beliefs, and maintaining reality testing. ASR3 can be understood as the implicit prior structure of internal object relations: the background expectation that relationships will soothe, abandon, engulf, humiliate, or destroy. ASR1 can be understood as the primordial affective vulnerability that must be regulated before symbolic prediction can stabilise.
Personality Organisation and Defensive Structure
Personality organisation is not reducible to trait description. While DSM-5-TR categories remain clinically and administratively important American Psychiatric Association, psychodynamic theory has long emphasised the structural dimensions of personality: identity integration, object relations, defensive organisation, reality testing, affect regulation, and superego functioning [18,19,27].
From an ASR perspective, personality organisation may be conceptualised as the stabilised adult form of early ASR configurations. Narcissistic, borderline, avoidant, dependent, schizoid, histrionic, echoistic, or compulsively compliant formations may all be explored not as fixed essences, but as structural adaptations to early affective and relational conditions. This does not remove diagnostic distinctions. Rather, it asks what underlying ASR configuration produces the observable pattern.
For example, borderline organisation may involve unstable ASR2 mediation under high relational threat, with rapid activation of ASR1 terror and ASR3 splitting. Narcissistic organisation may involve rigid defensive ASR2-like control built upon persecutory or shame-saturated ASR3 structures and intolerable ASR1 vulnerability. Avoidant or schizoid adaptations may involve reduced relational approach as a defence against ASR1 overwhelm and ASR3 threat expectation. Dependent or echoistic adaptations may involve chronic outsourcing of ASR2 stability to external objects, with self-erasure functioning as a strategy for preventing rupture. These are theoretical mappings rather than validated diagnostic claims. Their value lies in generating a structural language for exploring how surface personality patterns may emerge from deeper regulatory architectures.
Collapse, Consciousness, and Near-Death Phenomenology
The ASR model also draws cautiously on collapse and near-death phenomenology. Studies of cardiac arrest, dying brain activity, and near-death experiences have raised important questions about consciousness, selfhood, memory, and terminal neurophysiology [28-33]. More recent work has continued to examine gamma activity, neurophysiological coupling, and the limits of interpretation in dying or near-dying states [34,35].
This material must not be overstated. Near-death literature does not prove the ASR model. It does, however, provide comparative material for thinking about self-dissolution, altered consciousness, memory surge, ego collapse, and the layered organisation of self-experience. MPIT uses this literature inferentially to propose that collapse may proceed through a reversal of developmental organisation.
In developmental formation, the model proposes ASR1 → ASR3 → ASR2. In collapse or regression, it proposes ASR2 → ASR3 → ASR1.
This remains a theoretical proposition requiring empirical testing.
Positioning the ASR Complex Within Existing Literature
The ASR Complex builds upon attachment theory by preserving the importance of early caregiving while shifting the explanatory focus from behavioural classification to structural organisation. It builds upon object relations by locating internal objects, introjects, splitting, and object constancy within ASR3 and ASR2 dynamics. It builds upon affect regulation and trauma theory by treating early dysregulation not only as symptom formation but as gate formation. It builds upon predictive processing by conceptualising the self as an anticipatory system whose internal models may become organised around safety, rupture, shame, or annihilation.
The ASR Complex differs from existing models by proposing a tripartite architecture linking affective vulnerability, internal object organisation, and predictive reality mediation. It advances the discussion by offering a conceptual bridge between attachment behaviour, internal object relations, trauma response, personality organisation, and collapse vulnerability. This bridge remains theoretical, but it may provide a useful framework for research, clinical formulation, and future assessment development.
The ASR Complex: Core Theoretical Model
ASR1 / ASR-1: Primordial Affective Vulnerability
ASR1 refers to the earliest affective field of the organism. It is pre-symbolic, somatic, dependent, and prior to stable self-other differentiation. In infancy, ASR1 is expressed through hunger, distress, arousal, need, discomfort, and the requirement for external regulation. It is not yet mediated by reflective thought or symbolic meaning. It is the raw vulnerability of being alive before the self can organise experience.
In healthy development, ASR1 is held through caregiver attunement. The caregiver’s timing, tone, touch, gaze, rhythm, and repair help transform unregulated affect into survivable affect. Under these conditions, the infant gradually learns that arousal can rise and fall without annihilation.
When ASR1 is repeatedly unheld, misattuned, shamed, neglected, or frightened, affect may become associated with danger, shame, or collapse.
ASR1 is therefore not pathological in itself. It becomes clinically significant when the organism learns that its own affective aliveness is unsafe.
ASR3 / ASR-3: Internal Object World and Symbolic Unconscious
ASR3 refers to the unconscious internal object world. It includes internalised caregiver patterns, introjects, implicit relational expectations, affective memories, shame templates, threat predictions, safety models, and the early organisation of good and bad object images.
ASR3 is not simply repressed content. It is the relational blueprint beneath conscious prediction. It stores the patterned meanings of early experience: whether need is met, whether anger destroys connection, whether absence can be survived, whether shame is annihilating, whether care is reliable, and whether the self is welcome or dangerous.
In object-relations terms, ASR3 is the field in which splitting, introjection, exciting objects, rejecting objects, persecutory objects, and good-enough objects become organised. In predictive-processing terms, ASR3 may be understood as the implicit prior structure through which future relational experience is anticipated.
ASR2 / ASR-2: Predictive Ego and Reality-Mediating Gate
ASR2 refers to the mature predictive ego and reality-mediating gate. It is the layer of selfhood capable of symbolic delay, mentalisation, object constancy, ambiguity tolerance, reflective function, narrative continuity, and reality testing.
Where ASR1 feels and ASR3 remembers, ASR2 mediates. It allows the subject to experience affect without becoming affect, to hold mixed representations of self and other, to tolerate absence without collapse, and to revise expectation in light of reality. ASR2 is therefore central to adult attachment security, psychological flexibility, and integrated personality organisation.
In MPIT, the Organising Gate refers to the reality-mediation interface through which bodily signal, affective arousal, internal object activation, and symbolic interpretation are integrated into a coherent experience of reality. ASR2 is the mature form of that gate.
Developmental Sequence
MPIT proposes the following developmental construction sequence:
ASR1 → ASR3 → ASR2
In this sequence, the infant begins in ASR1: undifferentiated affective vulnerability. Through repeated relational experience, ASR3 develops as the internal object world, storing patterns of attunement, rupture, repair, shame, threat, and safety. ASR2 emerges later as the predictive ego: the reflective, reality-mediating structure capable of organising internal experience into coherent selfhood.
This developmental sequence reframes attachment as the construction of a layered regulatory architecture. Attachment behaviours are not merely learned responses. They are the behavioural outputs of ASR2 strategies built upon ASR3 predictions and organised around ASR1 vulnerability.
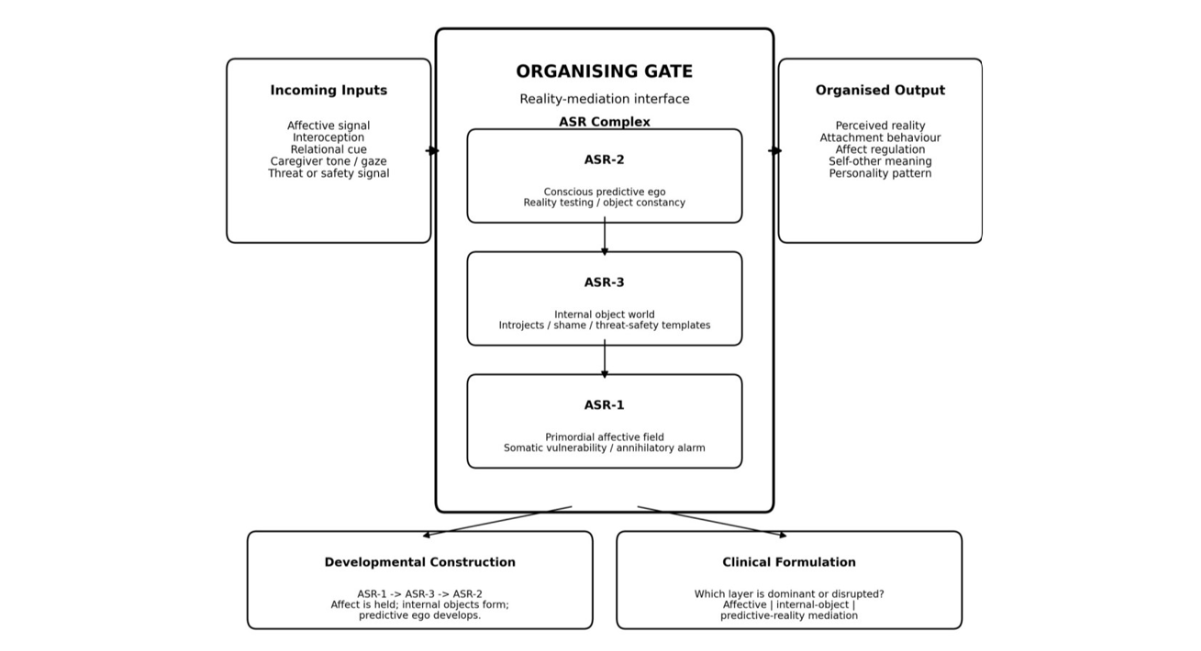
Figure 1: The ASR Complex as Organising Gate
Note: MPIT Proposes the ASR Complex as a layered organising architecture through which affective, interoceptive and relational input are mediated into coherent reality, attachment behaviour, affect regulation, self-other meaning and personality organization.
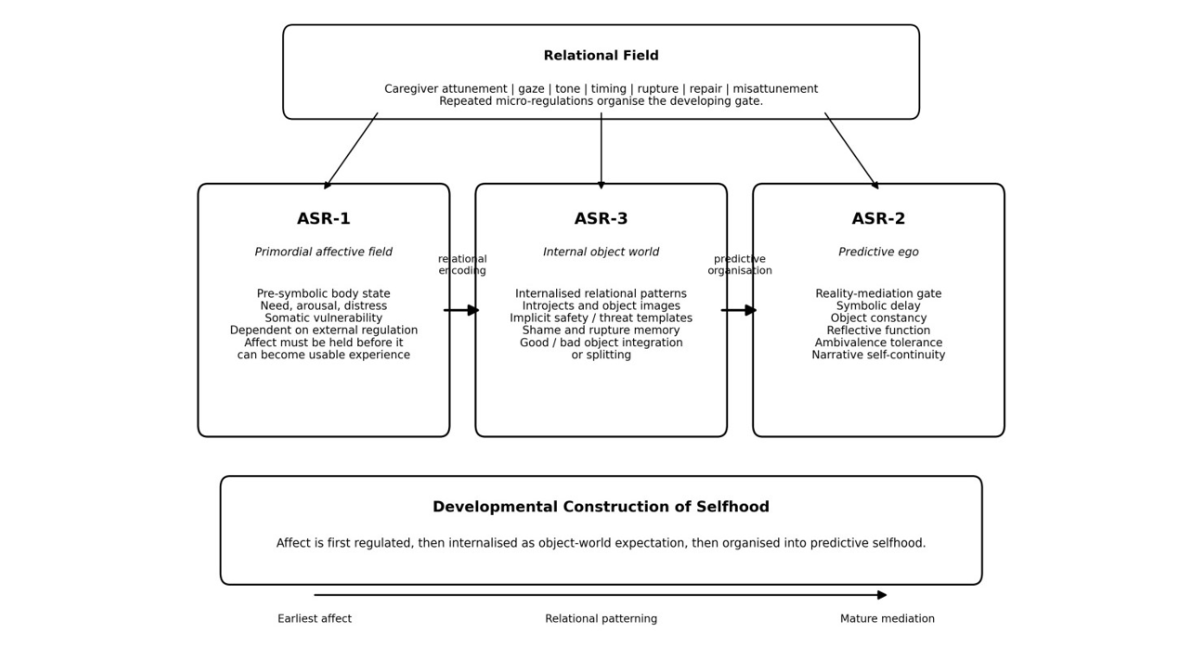
Figure 2: Developmental Construction Sequence: ASR1 → ASR3 → ASR2
Note: MPIT proposes that development proceeds from ASR-1 to ASR-3 to ASR-2: primordial affective vulnerability is first externally regulated, then encoded into the internal object world, and finally organised into a mature predictive ego capable of reality mediation.
Collapse Sequence
MPIT proposes that collapse or regression may follow the reverse sequence: ASR2 → ASR3 → ASR1
When ASR2 fails under relational stress, trauma, shame, abandonment, or symbolic rupture, the subject may lose reflective capacity, narrative continuity, object constancy, and reality-testing stability. ASR3 may then surge in the form of internal object activation: persecutory introjects, shame states, traumatic memory, splitting, fantasy, or dissociative symbolic material. If collapse deepens further, ASR1 may become dominant: raw affective terror, somatic overwhelm, annihilatory panic, or preverbal dysregulation.
This sequence is a theoretical proposition. It is not presented as a proven neurobiological law. However, it offers a clinically useful model for understanding why relational rupture may produce not only sadness or grief, but temporary failures of self-coherence, symbolic mediation, and affect regulation.
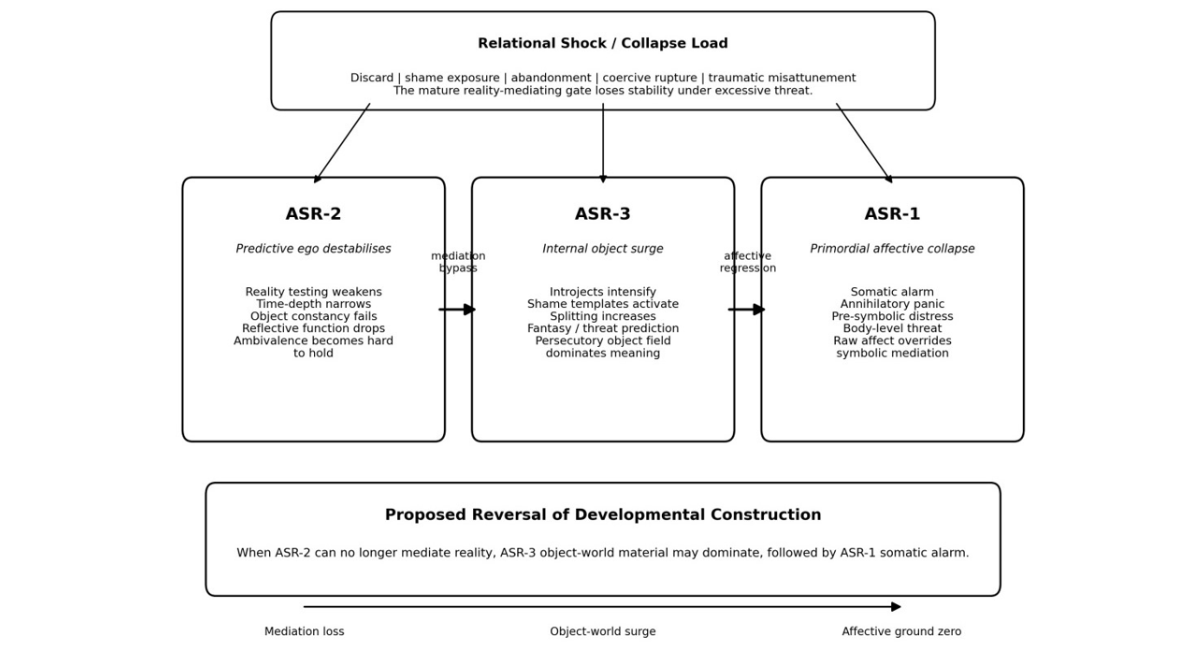
Figure 3: Collapse Reversal Sequence: ASR2 → ASR3 → ASR1
Note: MPIT proposes that collapse or regression may proceed in reverse order of development: ASR-2 destabilises first, ASR-3 internal-object material then becomes dominant, and ASR-1 may finally emerge as raw somatic alarm or annihilatory affect. This sequence is theoretical and requires empirical validation.
RESULTS
Attachment as ASR Configuration
The central conceptual finding of this synthesis is that attachment styles may be reframed as behavioural expressions of deeper ASR configurations. Secure, anxious, avoidant, and disorganised patterns are not discarded. Rather, they are reinterpreted as visible strategies produced by different relationships between ASR1 vulnerability, ASR3 internal object organisation, and ASR2 predictive mediation.
This reframing allows attachment to be understood as structural rather than merely behavioural. The child does not simply develop a “style.” The child develops an internal architecture for managing affect, expectation, absence, rupture, and relational uncertainty.
Secure Attachment as Integrated ASR Development
Secure attachment may be conceptualised as integrated ASR development. In this configuration, ASR1 has been sufficiently held; ASR3 contains coherent and reparative internal object patterns; and ASR2 develops as a flexible, reality-based mediator of affect and relationship.
The securely attached subject can experience distress without psychic collapse, maintain object constancy under absence, hold ambivalence without splitting, and use relational repair to update expectation. This does not mean the absence of pain or conflict. It means the presence of an internal architecture capable of metabolising rupture without disintegration.
Insecure Attachment as Partial ASR Distortion
Insecure attachment may be conceptualised as partial ASR distortion. In anxious configurations, ASR1 vulnerability may remain highly exposed, ASR3 may contain inconsistent or unreliable object patterns, and ASR2 may become hyperactivated around proximity-seeking, reassurance, and threat detection. In avoidant configurations, ASR2 may develop strategies of deactivation, minimisation, and self-sufficiency in order to reduce exposure to ASR1 vulnerability and ASR3 disappointment. In disorganised configurations, ASR3 may contain contradictory or frightening object representations that ASR2 cannot integrate, resulting in collapse, contradiction, or approach-avoidance patterns under stress.
This model does not replace established attachment classifications. It provides a proposed structural account of how those classifications may be generated.
Personality Organisation as Stabilised ASR Architecture
A further conceptual finding is that personality organisation may be understood as stabilised ASR architecture. Repeated relational patterns do not simply produce temporary behaviours; over time, they may organise the person’s enduring ways of regulating affect, anticipating others, defending against shame, maintaining self-continuity, and managing internal objects.
Narcissistic, borderline, avoidant, dependent, schizoid, echoistic, or compulsively compliant formations may therefore be explored as different ASR outcomes. This does not mean that these formations are identical, nor that diagnostic distinctions are irrelevant. It means that personality structure can be investigated in terms of which ASR layer is dominant, which layer is underdeveloped, and which layer becomes defensive under threat.
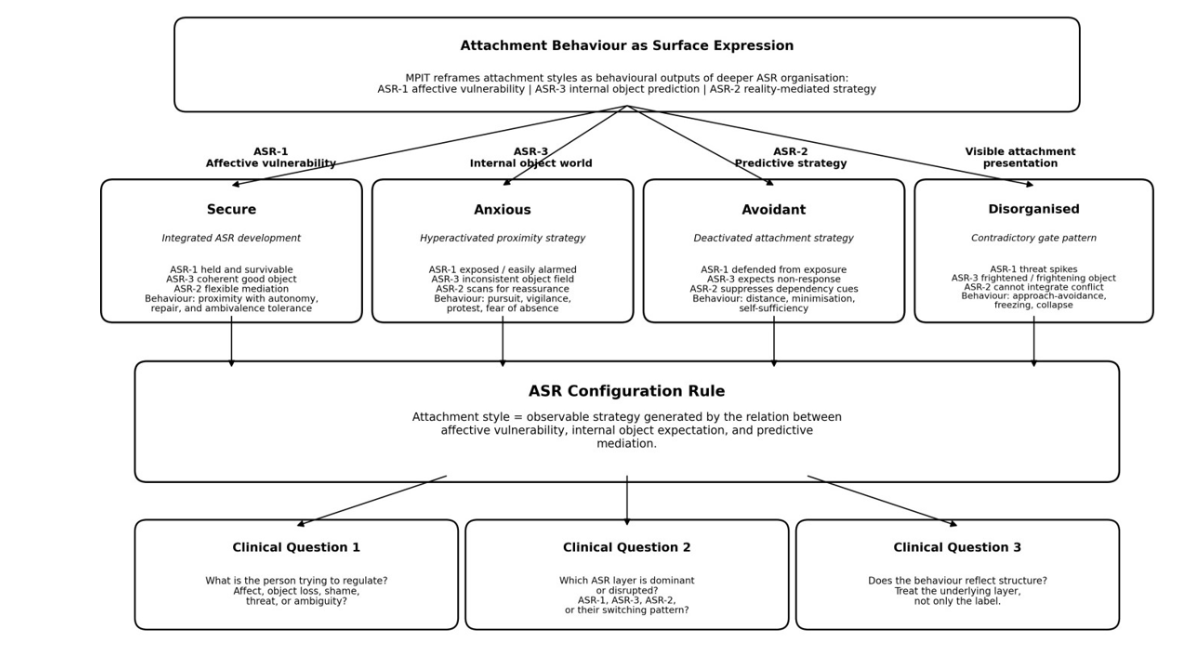
Figure 4: Attachment Styles as ASR Configurations.
Note: The figure does not replace standard attachment classifications. It shows how MPIT positions secure, anxious, avoidant, and disorganised patterns as behavioural signatures of underlying ASR configurations.
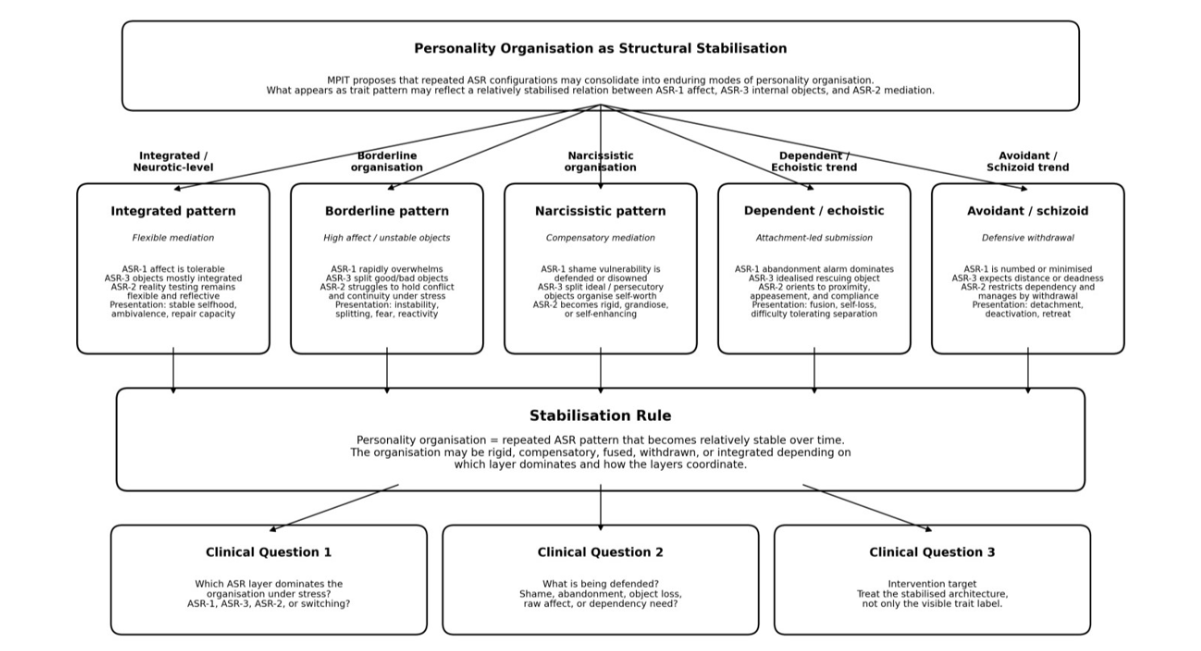
Figure 5: Personality Organisation as Stabilised ASR Architecture
Note: The figure is conceptual, not diagnostic. The listed patterns are illustrative examples of how MPIT positions personality organisation as stabilised ASR architecture rather than as a mere trait collection.
Clinical Implication: Treating the Layer, Not the Label
The clinical implication of the synthesis is that intervention should target the disrupted ASR layer rather than only the surface label. If ASR1 is dominant, treatment may need to prioritise somatic stabilisation, containment, grounding, and reduction of arousal. If ASR2 is impaired or bypassed, treatment may need to strengthen mentalisation, reflective capacity, object constancy, time-depth, narrative coherence, and ambiguity tolerance. If ASR3 is dominant, treatment may need to address introjects, internal objects, shame structures, implicit relational templates, dissociation, and splitting.
Thus, the question is not only “What attachment style does this person show?” but “Which ASR layer is organising the person’s reality under stress?”
Clinical and Developmental Implications
The ASR Complex may help clinicians distinguish surface behaviour from underlying structure. Two clients may both present as anxious, avoidant, dependent, narcissistic, or emotionally dysregulated, yet the underlying ASR organisation may differ significantly. One may be dominated by ASR1 somatic terror, another by ASR3 persecutory introjects, and another by a brittle ASR2 strategy that collapses under shame or abandonment.
Attachment labels alone may therefore be insufficient for clinical formulation. They describe behavioural tendencies, but they do not always identify whether the client requires affective stabilisation, mentalisation work, internal object interpretation, shame processing, dissociation treatment, or reconstruction of narrative continuity.
ASR1 disruption may require interventions that stabilise the body before interpretation is attempted. These may include grounding, breath regulation, somatic tracking, containment, sensory regulation, and relational safety. In ASR1 states, insight may be unavailable because the system is organised around immediate survival rather than reflective meaning.
ASR2 disruption may require work with mentalisation, narrative coherence, object constancy, symbolic delay, and reflective function. The therapeutic task is to strengthen the client’s ability to hold affect, time, contradiction, and relational ambiguity without immediate collapse into action, fantasy, splitting, or self-erasure.
ASR3 disruption may require sustained work with internal objects, introjects, shame, implicit relational templates, dissociation, and persecutory self-states. The therapist may need to help the client identify which internal object configuration has become active, how it shapes prediction, and how it distorts current relational experience.
The clinical principle is layer-specific intervention. Treatment should ask: Is the presenting problem primarily affective, predictive, or internal-object based? Is the client overwhelmed by ASR1, bypassing ASR2, or organised by ASR3? What must be stabilised before interpretation can be useful?
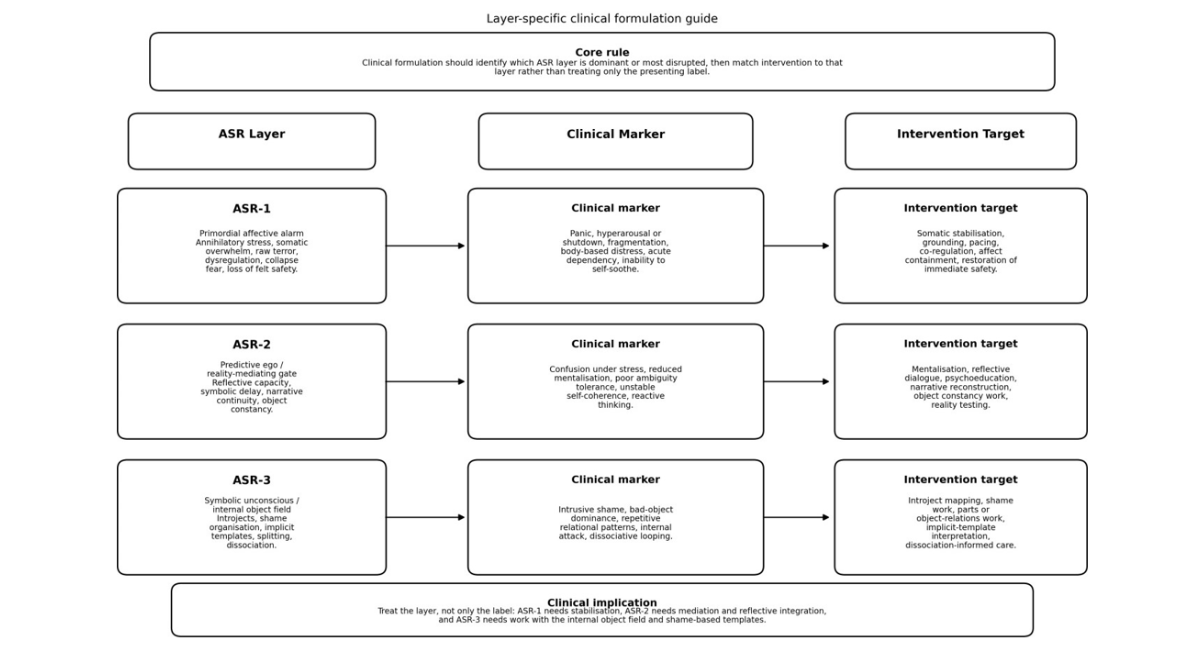
Figure 6: ASR Layer → Clinical Marker → Intervention Target
DISCUSSION
The ASR Complex reframes attachment theory by shifting the central question from behavioural classification to structural organisation. Attachment categories remain useful, but they may be understood as surface expressions of a deeper regulatory architecture. The secure child is not merely behaving securely; the child has developed an internal structure in which affect can be held, internal objects remain coherent, and reality can be mediated flexibly. The insecure or disorganised child is not merely displaying maladaptive behaviour; the child may be expressing a disrupted relationship between affective vulnerability, internal object expectation, and predictive self-organisation.
The model integrates attachment theory, object relations, trauma theory, affect regulation, and predictive processing by assigning each domain a structural place. Attachment describes relational behaviour and internal working models. Object relations describes the internal object world, splitting, introjection, false self organisation, and object constancy. Trauma theory describes dysregulation, dissociation, and disturbance in self-organisation under threat. Predictive processing describes the anticipatory and embodied nature of perception, affect, and action. The ASR Complex proposes a framework through which these domains can be organised into a single layered model.
The model advances beyond behavioural classification by suggesting that attachment behaviour is an output of ASR configuration. In this sense, the same outward behaviour may have different structural meanings. Withdrawal may reflect avoidant deactivation, schizoid retreat, shame-based collapse, dissociative protection, or ASR3 threat expectation. Pursuit may reflect anxious attachment, dependency, narcissistic supply-seeking, echoistic self-erasure, or ASR1 panic. Clinical formulation therefore requires more than behavioural description.
The ASR Complex also contributes to personality development theory. It suggests that adult personality organisation may reflect the stabilised outcome of early ASR development.
Narcissistic, borderline, echoistic, avoidant, dependent, schizoid, and related formations can be explored as different structural solutions to affective vulnerability, internal object contradiction, and predictive instability. This avoids reducing personality to traits alone while also avoiding moralising or overly simplistic developmental explanations.
However, several aspects of the model remain speculative. The ASR Complex has not yet been operationalised as a validated clinical instrument. Its three layers require clearer measurement criteria. Its developmental and collapse sequences require longitudinal, neurobiological, and clinical testing. The proposed relationship between near-death phenomenology, collapse, and ASR reversal is inferential and should not be treated as direct evidence. Similarly, the mapping of personality configurations onto ASR architecture remains theoretical and must be tested against existing attachment, trauma, and personality measures.
The model should therefore be understood as a conceptual framework, not a diagnostic system. Its primary value at this stage is heuristic. It provides a language for asking more precise clinical questions: What is being regulated? Which internal object is active? Is the client in affective terror, predictive collapse, or internal-object domination? Is the apparent attachment style actually a deeper ASR configuration? These questions may help refine formulation and guide future research.
RECOMMENDATIONS
Researchers should operationalise ASR1, ASR2, and ASR3 into measurable constructs. Each layer requires clear markers, assessment criteria, and testable hypotheses.
Clinicians should assess whether attachment symptoms reflect affective disruption, predictive disruption, or internal-object disruption. The same behavioural presentation may require different interventions depending on the ASR layer involved.
Future attachment research should distinguish behavioural style from structural organisation. Attachment classifications may be strengthened by integrating measures of affect regulation, internal object coherence, reflective function, interoceptive prediction, and defensive structure.
Clinical training should include mapping between affect regulation, internal objects, and predictive self-organisation. This may help clinicians avoid treating all attachment insecurity as the same phenomenon.
The ASR model should be tested alongside existing attachment, trauma, personality, and dissociation measures. Its value will depend on whether it can explain clinical variation not already captured by existing instruments.
Areas for Further Research
Further research should focus on empirical validation of ASR constructs. ASR1, ASR2, and ASR3 require operational definitions that can be tested in clinical and non-clinical populations.
An ASR assessment scale should be developed to identify dominant ASR configurations, collapse patterns, and layer-specific disruptions.
Future studies should compare ASR configurations with established attachment classifications, including secure, anxious, avoidant, and disorganised patterns.
Research should examine the relationship between ASR patterns and personality disorder presentations, including narcissistic, borderline, avoidant, dependent, schizoid, and related structures.
The relationship between ASR and complex trauma requires further study, particularly in relation to affect dysregulation, dissociation, shame, and disturbances in self-organisation.
ASR mapping may be especially relevant in survivors of narcissistic abuse, coercive control, relational trauma, and shared fantasy collapse.
Longitudinal studies should examine how caregiver attunement, rupture, repair, shame, neglect, and frightening caregiving influence ASR development across infancy, childhood, adolescence, and adulthood.
Neurobiological research should investigate possible relationships between ASR configurations, interoception, prediction error, affect regulation, prefrontal-limbic functioning, and autonomic regulation.
Cross-cultural validation is necessary. Concepts such as selfhood, attachment, shame, autonomy, dependency, and caregiving vary across cultures, and ASR theory must not assume universal expression without testing.
Clinical outcome studies should examine whether ASR-informed formulation improves therapeutic alliance, treatment targeting, affect regulation, and recovery from relational trauma.
LIMITATIONS
The ASR Complex is currently a theoretical model. It has not yet been validated as an empirical construct, diagnostic tool, or standardised clinical assessment.
This manuscript is a conceptual synthesis, not an empirical study. It does not present original data, statistical analysis, systematic review methodology, or meta-analytic findings.
The model requires operationalisation. ASR1, ASR2, and ASR3 must be translated into measurable clinical, behavioural, phenomenological, and neurobiological indicators.
Some claims require longitudinal, neurobiological, and clinical validation. In particular, the proposed developmental sequence ASR1 → ASR3 → ASR2 and collapse sequence ASR2 → ASR3 → ASR1 remain theoretical propositions.
The use of near-death and collapse literature is comparative and inferential. It should not be interpreted as direct proof of ASR architecture.
Cultural generalisability must be tested. The ASR Complex has been developed within a Western psychodynamic and trauma-theoretical context, and its applicability across cultures requires careful examination.
CONCLUSION
The ASR Complex is proposed as an integrative framework linking attachment, affect regulation, object relations, predictive processing, trauma, and personality organisation. It reframes attachment styles as surface expressions of deeper regulatory architecture and proposes that personality organisation reflects stabilised ASR configurations formed through early relational experience.
Within this model, ASR1 represents primordial affective vulnerability, ASR3 represents the internal object world and symbolic unconscious, and ASR2 represents the mature predictive ego and reality-mediating gate. Development is proposed to proceed through ASR1 → ASR3 → ASR2, while collapse or regression may proceed through the reverse sequence: ASR2 → ASR3 → ASR1.
The model’s clinical value lies in its capacity to distinguish affective, predictive, and internal-object disruptions beneath surface attachment labels. While requiring empirical validation, the ASR Complex may offer a useful structural language for understanding development, collapse, personality organisation, and therapeutic reconstruction.
REFERENCES
- Ainsworth MD, Blehar MC, Waters E, Wall SN. Patterns of attachment: A psychological study of the strange situation. Psychology press; 2015. [Google Scholar]
- Bowlby J. Attachment and loss, vol. II: Separation. Basic Books; 1973. [Google Scholar]
- Altschul S. Attachment and Loss, Vol. 3. Loss, Sadness and Depression. By John Bowlby. Journal of the American Psychoanalytic Association. 1984 Feb;32(1):216-8. [Google Scholar]
- Bowlby J. Attachment and loss v. 3 (Vol. 1). [Google Scholar]
- Main M, Solomon J. Procedures for identifying infants as disorganized/disoriented during the Ainsworth Strange Situation. Attachment in the preschool years: Theory, research, and intervention. 1990;1:121-60. [Google Scholar]
- Gillath, O., Karantzas, G. C., Selcuk, E., & Adams, G. C. (2022). Attachment security priming: A meta-analysis. Personality and Social Psychology Review, 26(3), 183–241. [Crossref] [Google Scholar] [PubMed]
- Park Y, Impett EA, MacDonald G, Lemay Jr EP. Saying “thank you”: Partners’ expressions of gratitude protect relationship satisfaction and commitment from the harmful effects of attachment insecurity. Journal of personality and social psychology. 2019;117(4):773. [Crossref] [Google Scholar] [PubMed]
- Beare, M. T. (2026). The ASR Complex, Personality & Attachment. MPIT Research Institute.
- Barrett LF. How emotions are made: The secret life of the brain. Pan Macmillan; 2017. [Google Scholar]
- Clark A. Surfing uncertainty: Prediction, action, and the embodied mind. Oxford University Press; 2015. [Google Scholar]
- Friston K. The free-energy principle: a unified brain theory? Nature reviews neuroscience. 2010;11(2):127-38. [Crossref] [Google Scholar] [PubMed]
- Hohwy J. The Predictive Mind Oxford, UK: Oxford Univ. [Google Scholar]
- Seth AK, Friston KJ. Active interoceptive inference and the emotional brain. Philosophical Transactions of the Royal Society B: Biological Sciences. 2016;371(1708). [Crossref] [Google Scholar] [PubMed]
- Putica A, Agathos J. Reconceptualizing complex posttraumatic stress disorder: A predictive processing framework for mechanisms and intervention. Neuroscience & Biobehavioral Reviews. 2024;164:105836. [Crossref] [Google Scholar] [PubMed]
- Fairbairn WR. Psychoanalytic studies of the personality. Psychology Press; 1994. [Crossref] [Google Scholar]
- Klein M. Notes on some schizoid mechanisms. In Influential Papers from the 1940s. 2018 (pp. 337-364). Routledge. [Crossref] [Google Scholar] [PubMed]
- Winnicott DW. Ego distortion in terms of true and false self. In The person who is me 2018. (pp. 7-22). Routledge. [Crossref] [Google Scholar]
- Winnicott DW. The maturational processes and the facilitating environment: Studies in the theory of emotional development. The International Psycho-Analytic Library. 1965;64:1-276. [Google Scholar]
- Kernberg OF. Borderline conditions and pathological narcissism. [Crossref] [Google Scholar]
- Kernberg OF. Severe personality disorders: Psychotherapeutic strategies. Yale University Press; 1993. [Google Scholar]
- Schore AN. Affect Regulation and the Repair of the Self. The Permanente 2005;9(2). [Google Scholar]
- Schore AN. The science of the art of psychotherapy. WW Norton & Company; 2012. [Google Scholar]
- Van der Kolk B. The body keeps the score: Brain, mind, and body in the healing of trauma. New York. 2014;3:14-211. [Google Scholar]
- Fonagy P, Gergely G, Jurist EL. Affect regulation, mentalization and the development of the self. Routledge; 2018. [Crossref] [Google Scholar]
- Bateman A, Fonagy P, Campbell C, Luyten P, Debbané M. Cambridge guide to mentalization-based treatment (MBT). Cambridge University Press; 2023. [Crossref] [Google Scholar]
- Lee KM, Ferreira-Santos F, Satpute AB. Predictive processing models and affective neuroscience. Neuroscience & Biobehavioral Reviews. 2021;131:211-28. [Crossref] [Google Scholar] [PubMed]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th edn VA: American Psychiatric Publishing. 2013;10. [Crossref] [Google Scholar]
- Borjigin J, Lee U, Liu T, Pal D, Huff S, Klarr D, et al. Surge of neurophysiological coherence and connectivity in the dying brain. Proceedings of the National Academy of Sciences. 2013;110(35):14432-7. [Crossref] [Google Scholar] [PubMed]
- Chawla LS, Akst S, Junker C, Jacobs B, Seneff MG. Surges of electroencephalogram activity at the time of death: a case series. Journal of palliative medicine. 2009;12(12):1095-100. [Crossref] [Google Scholar] [PubMed]
- Greyson B. Incidence and correlates of near-death experiences in a cardiac care unit. General hospital psychiatry. 2003;25(4):269-76. [Crossref] [Google Scholar] [PubMed]
- Martial C, Cassol H, Charland-Verville V, Pallavicini C, Sanz C, Zamberlan F, et al. Neurochemical models of near-death experiences: A large-scale study based on the semantic similarity of written reports. Consciousness and cognition. 2019;69:52-69. [Crossref] [Google Scholar] [PubMed]
- Martial C, Simon J, Puttaert N, Gosseries O, Charland-Verville V, Nyssen AS, et al. The Near-Death Experience Content (NDE-C) scale: development and psychometric validation. Consciousness and Cognition. 2020;86:103049. [Crossref] [Google Scholar] [PubMed]
- Parnia S, Spearpoint K, De Vos G, Fenwick P, Goldberg D, Yang J, et al. AWARE—AWAreness during REsuscitation—A prospective study. Resuscitation. 2014;85(12):1799-805. [Crossref] [Google Scholar]
- Xu G, Mihaylova T, Li D, Tian F, Farrehi PM, Parent JM, et al. Surge of neurophysiological coupling and connectivity of gamma oscillations in the dying human brain. Proceedings of the National Academy of Sciences. 2023 ;120(19):e2216268120. [Crossref] [Google Scholar] [PubMed]
- Shaw NA. The gamma-band activity model of the near-death experience: a critique and a reinterpretation. F1000Research. 2024;13:674. [Crossref] [Google Scholar] [PubMed]
Article Processing Timeline
| 2-5 Days | Initial Quality & Plagiarism Check |
| 25-35 Days |
Peer Review Feedback |
| 45-60 Days | Total article processing time |
Ethics & Policies
Editorial & Management
Useful Links
Journal Highlights
Open Access Journals
Membership
Journal Flyer